

PKD2-Related Autosomal Dominant Polycystic Kidney Disease: Prevalence, Clinical Presentation, Mutation Spectrum, and Prognosis
- PMID: 28356211
- PMCID: PMC5610929
- DOI: 10.1053/j.ajkd.2017.01.046
PKD2-Related Autosomal Dominant Polycystic Kidney Disease: Prevalence, Clinical Presentation, Mutation Spectrum, and Prognosis
Abstract
Background: PKD2-related autosomal dominant polycystic kidney disease (ADPKD) is widely acknowledged to be of milder severity than PKD1-related disease, but population-based studies depicting the exact burden of the disease are lacking. We aimed to revisit PKD2 prevalence, clinical presentation, mutation spectrum, and prognosis through the Genkyst cohort.
Study design: Case series, January 2010 to March 2016.
Settings & participants: Genkyst study participants are individuals older than 18 years from 22 nephrology centers from western France with a diagnosis of ADPKD based on Pei criteria or at least 10 bilateral kidney cysts in the absence of a familial history. Publicly available whole-exome sequencing data from the ExAC database were used to provide an estimate of the genetic prevalence of the disease.
Outcomes: Molecular analysis of PKD1 and PKD2 genes. Renal survival, age- and sex-adjusted estimated glomerular filtration rate.
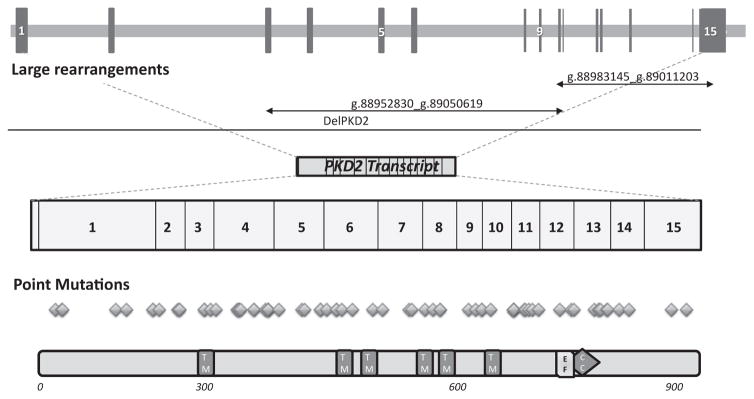
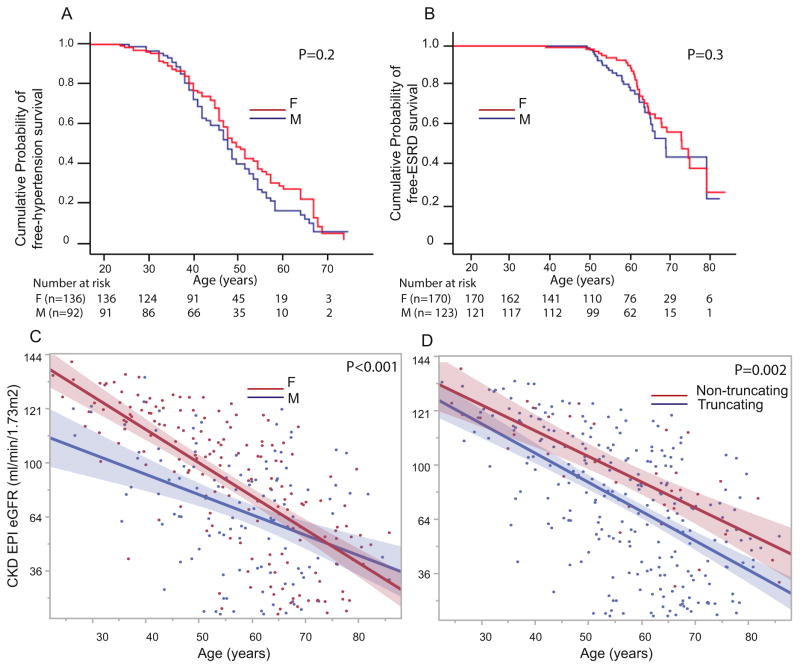
Results: The Genkyst cohort included 293 patients with PKD2 mutations (203 pedigrees). PKD2 patients with a nephrology follow-up corresponded to 0.63 (95% CI, 0.54-0.72)/10,000 in Brittany, while PKD2 genetic prevalence was calculated at 1.64 (95% CI, 1.10-3.51)/10,000 inhabitants in the European population. Median age at diagnosis was 42 years. Flank pain was reported in 38.9%; macroscopic hematuria, in 31.1%; and cyst infections, in 15.3% of patients. At age 60 years, the cumulative probability of end-stage renal disease (ESRD) was 9.8% (95% CI, 5.2%-14.4%), whereas the probability of hypertension was 75.2% (95% CI, 68.5%-81.9%). Although there was no sex influence on renal survival, men had lower kidney function than women. Nontruncating mutations (n=36) were associated with higher age-adjusted estimated glomerular filtration rates. Among the 18 patients with more severe outcomes (ESRD before age 60), 44% had associated conditions or nephropathies likely to account for the early progression to ESRD.
Limitations: Younger patients and patients presenting with milder forms of PKD2-related disease may not be diagnosed or referred to nephrology centers.
Conclusions: Patients with PKD2-related ADPKD typically present with mild disease. In case of accelerated degradation of kidney function, a concomitant nephropathy should be ruled out.
Keywords: Autosomal dominant polycystic kidney disease (ADPKD); PKD2; case series; disease progression; disease severity; end-stage renal disease (ESRD); genetic prevalence; genetics; kidney function; mutation detection; mutation spectrum; prognosis; renal survival; sequencing.
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Autosomal Dominant PKD in Patients With PKD2 Mutations-A Benign Disorder?Am J Kidney Dis. 2017 Oct;70(4):456-457. doi: 10.1053/j.ajkd.2017.06.009. Am J Kidney Dis. 2017. PMID: 28941485 No abstract available.
References
-
- Dalgaard OZ. Bilateral polycystic disease of the kidneys; a follow-up of two hundred and eighty-four patients and their families. Acta Med Scand Suppl. 1957;328:1–255. - PubMed
-
- Neumann HPH, Jilg C, Bacher J, et al. Epidemiology of autosomal-dominant polycystic kidney disease: an in-depth clinical study for south-western Germany. Nephrol Dial Transplant. 2013;28(6):1472–1487. - PubMed
-
- Patch C, Charlton J, Roderick PJ, Gulliford MC. Use of antihypertensive medications and mortality of patients with autosomal dominant polycystic kidney disease: a population-based study. Am J Kidney Dis. 2011;57(6):856–862. - PubMed
-
- Willey CJ, Blais JD, Hall AK, Krasa HB, Makin AJ, Czerwiec FS. Prevalence of autosomal dominant polycystic kidney disease in the European Union. Nephrol Dial Transplant. 2016 http://dx.doi.org/10.1093/ndt/gfw240. - DOI - PMC - PubMed
-
- The European Polycystic Kidney Disease Consortium. The polycystic kidney disease 1 gene encodes a 14 kb transcript and lies within a duplicated region on chromosome 16. The European Polycystic Kidney Disease Consortium. Cell. 1994;78(6):881–894. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
