

Adrenocortical carcinoma masquerading as Cushing's disease
- PMID: 28356253
- PMCID: PMC5372172
- DOI: 10.1136/bcr-2016-217519
Adrenocortical carcinoma masquerading as Cushing's disease
Abstract
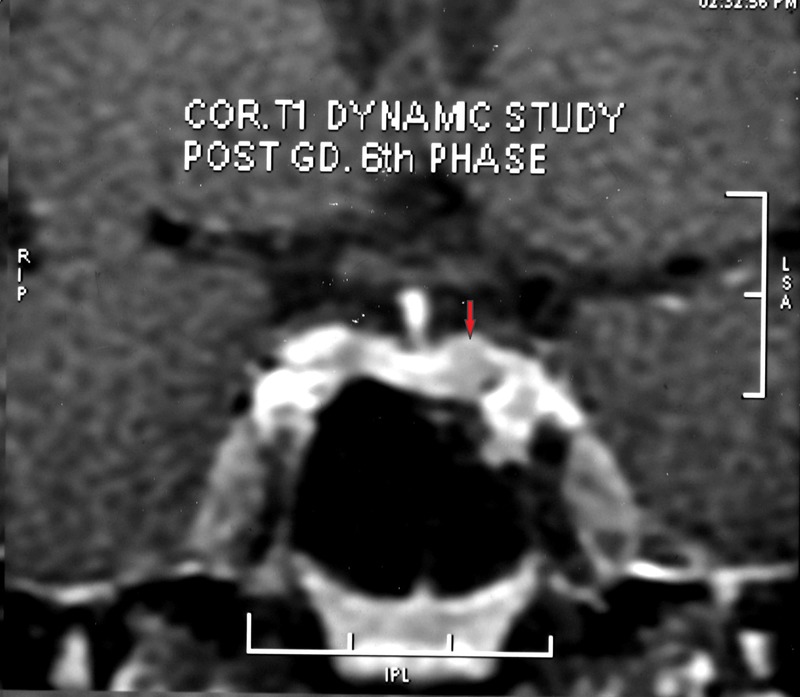
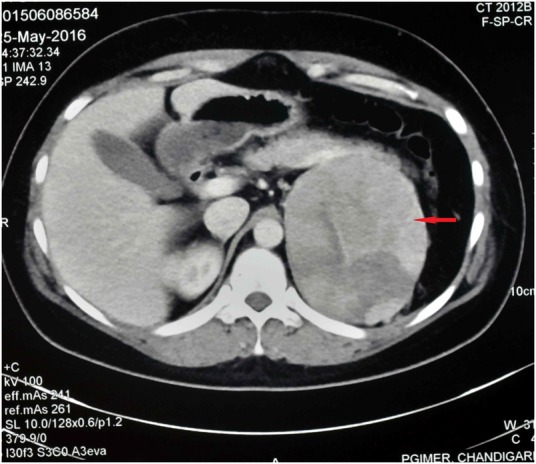
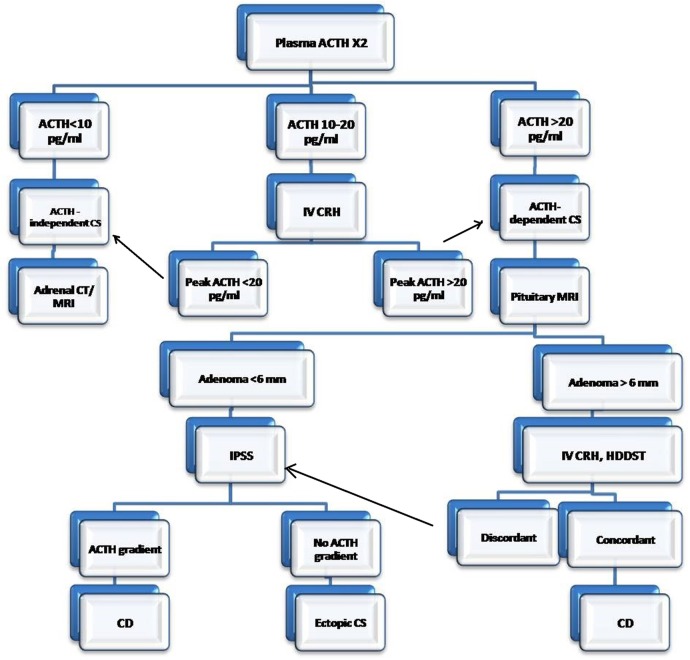
Cushing's syndrome (CS) can be classified as adrenocorticotropic hormone (ACTH)-dependent or ACTH-independent depending on the ACTH levels. However, 30% of the patients with CS have ACTH levels in the 'grey zone' (5-20 pg/mL), thereby posing a challenge in establishing the aetiological diagnosis. In a patient with full-blown features of Cushing's syndrome with equivocal ACTH levels, and a pituitary microadenoma on contrast-enhanced MRI sella, can falsely lead to a diagnosis of Cushing's disease. Pituitary microadenoma, if <6 mm in size, may be an incidental finding (incidentaloma) in this scenario and can be present in ∼3-27% of the healthy population. Therefore, in a patient with CS with equivocal ACTH levels and a pituitary microadenoma, multiple samplings for ACTH and adrenal imaging should be performed to exclude ACTH-independent CS and if required, bilateral inferior petrosal sinus sampling to determine the source of ACTH excess.
2017 BMJ Publishing Group Ltd.
Conflict of interest statement
Figures
Similar articles
-
Routine inferior petrosal sinus sampling in the differential diagnosis of adrenocorticotropin (ACTH)-dependent Cushing's syndrome: early recognition of the occult ectopic ACTH syndrome.J Clin Endocrinol Metab. 1991 Aug;73(2):408-13. doi: 10.1210/jcem-73-2-408. J Clin Endocrinol Metab. 1991. PMID: 1649842
-
A critical analysis of the value of simultaneous inferior petrosal sinus sampling in Cushing's disease and the occult ectopic adrenocorticotropin syndrome.J Clin Endocrinol Metab. 1999 Feb;84(2):487-92. doi: 10.1210/jcem.84.2.5437. J Clin Endocrinol Metab. 1999. PMID: 10022405
-
[Cushing's syndrome: diagnostic exploration].Presse Med. 1994 Jan 8-15;23(1):43-8. Presse Med. 1994. PMID: 8127815 Review. French.
-
The role of inferior petrosal sinus sampling in the diagnostic localization of Cushing's disease.Neurosurg Focus. 2007;23(3):E2. doi: 10.3171/foc.2007.23.3.3. Neurosurg Focus. 2007. PMID: 17961020 Review.
-
Comparison of MRI techniques for detecting microadenomas in Cushing's disease.J Neurosurg. 2018 Apr;128(4):1051-1057. doi: 10.3171/2017.3.JNS163122. Epub 2017 Apr 28. J Neurosurg. 2018. PMID: 28452619
Cited by
-
Approach to the Patient: Diagnosis of Cushing Syndrome.J Clin Endocrinol Metab. 2022 Nov 23;107(11):3162-3174. doi: 10.1210/clinem/dgac492. J Clin Endocrinol Metab. 2022. PMID: 36036941 Free PMC article.
-
Low DHEAS Level: A Surrogate Marker of Adrenal Cushing Syndrome with Grey Zone ACTH Levels.Indian J Endocrinol Metab. 2023 Jul-Aug;27(4):365-367. doi: 10.4103/ijem.ijem_161_23. Epub 2023 Aug 28. Indian J Endocrinol Metab. 2023. PMID: 37867991 Free PMC article. No abstract available.
References
-
- Findling JW. Clinical application of new immunoradiometric assay for ACTH. Endocrinologist 1992;2:360–5. 10.1097/00019616-199211000-00003 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources