

The pathophysiology of chronic thromboembolic pulmonary hypertension
- PMID: 28356405
- PMCID: PMC9488693
- DOI: 10.1183/16000617.0112-2016
The pathophysiology of chronic thromboembolic pulmonary hypertension
Abstract
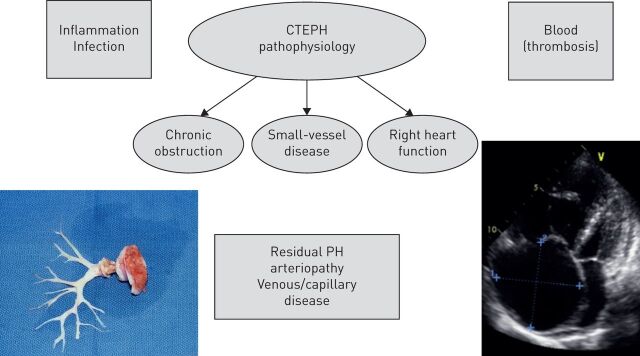
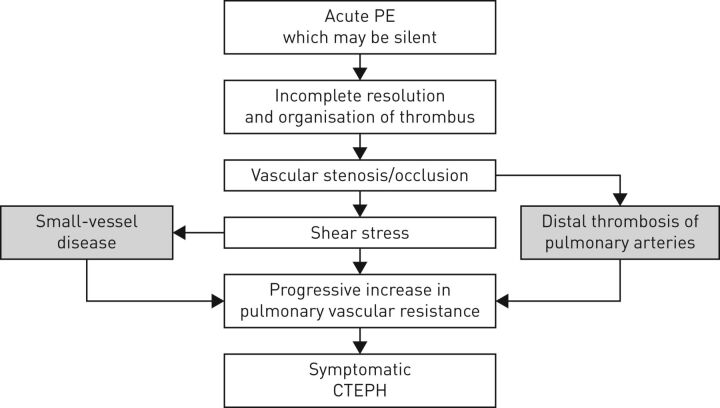
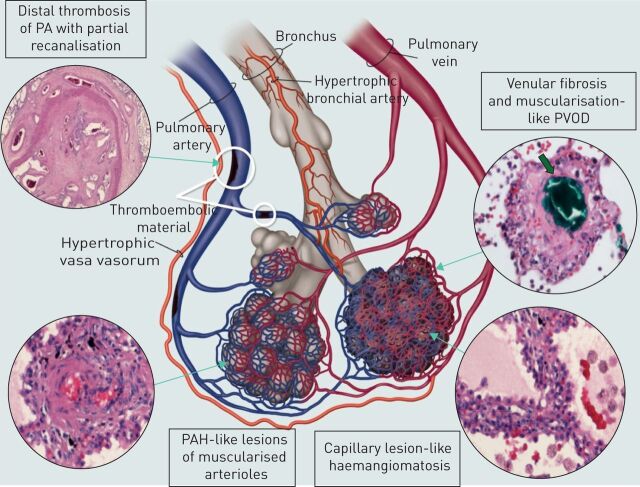
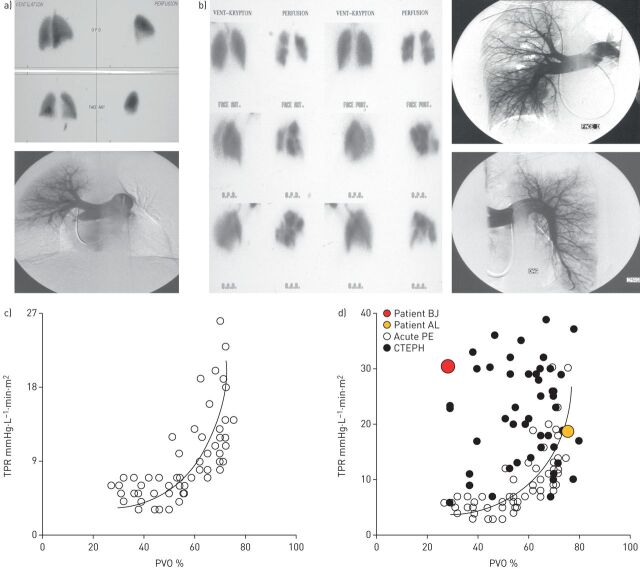
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare, progressive pulmonary vascular disease that is usually a consequence of prior acute pulmonary embolism. CTEPH usually begins with persistent obstruction of large and/or middle-sized pulmonary arteries by organised thrombi. Failure of thrombi to resolve may be related to abnormal fibrinolysis or underlying haematological or autoimmune disorders. It is now known that small-vessel abnormalities also contribute to haemodynamic compromise, functional impairment and disease progression in CTEPH. Small-vessel disease can occur in obstructed areas, possibly triggered by unresolved thrombotic material, and downstream from occlusions, possibly because of excessive collateral blood supply from high-pressure bronchial and systemic arteries. The molecular processes underlying small-vessel disease are not completely understood and further research is needed in this area. The degree of small-vessel disease has a substantial impact on the severity of CTEPH and postsurgical outcomes. Interventional and medical treatment of CTEPH should aim to restore normal flow distribution within the pulmonary vasculature, unload the right ventricle and prevent or treat small-vessel disease. It requires early, reliable identification of patients with CTEPH and use of optimal treatment modalities in expert centres.
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at
Figures

References
-
- Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013; 62: D34–D41. - PubMed
-
- Lang IM, Dorfmüller P, Vonk Noordegraaf A. The pathobiology of chronic thromboembolic pulmonary hypertension. Ann Am Thorac Soc 2016; 13: Suppl. 3, S215–S221. - PubMed
-
- Fedullo P, Kerr KM, Kim NH, et al. Chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med 2011; 183: 1605–1613. - PubMed
-
- Kim NH. Group 4 pulmonary hypertension: chronic thromboembolic pulmonary hypertension: epidemiology, pathophysiology, and treatment. Cardiol Clin 2016; 34: 435–441. - PubMed
-
- Pepke-Zaba J, Delcroix M, Lang I, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation 2011; 124: 1973–1981. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical