

ED misdiagnosis of cerebrovascular events in the era of modern neuroimaging: A meta-analysis
- PMID: 28356464
- PMCID: PMC5386439
- DOI: 10.1212/WNL.0000000000003814
ED misdiagnosis of cerebrovascular events in the era of modern neuroimaging: A meta-analysis
Abstract
Objective: With the emergency department (ED) being a high-risk site for diagnostic errors, we sought to estimate ED diagnostic accuracy for identifying acute cerebrovascular events.
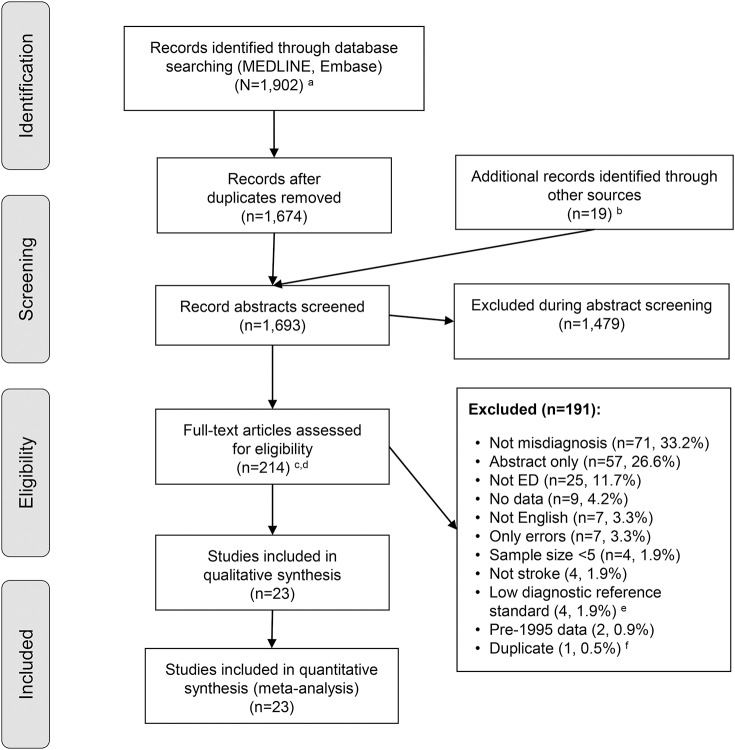
Methods: MEDLINE and Embase were searched for studies (1995-2016) reporting ED diagnostic accuracy for ischemic stroke, TIA, or subarachnoid hemorrhage (SAH). Two independent reviewers determined inclusion. We identified 1,693 unique citations, examined 214 full articles, and analyzed 23 studies. Studies were rated on risk of bias (QUADAS-2). Diagnostic data were extracted. We prospectively defined clinical presentation subgroups to compare odds of misdiagnosis.
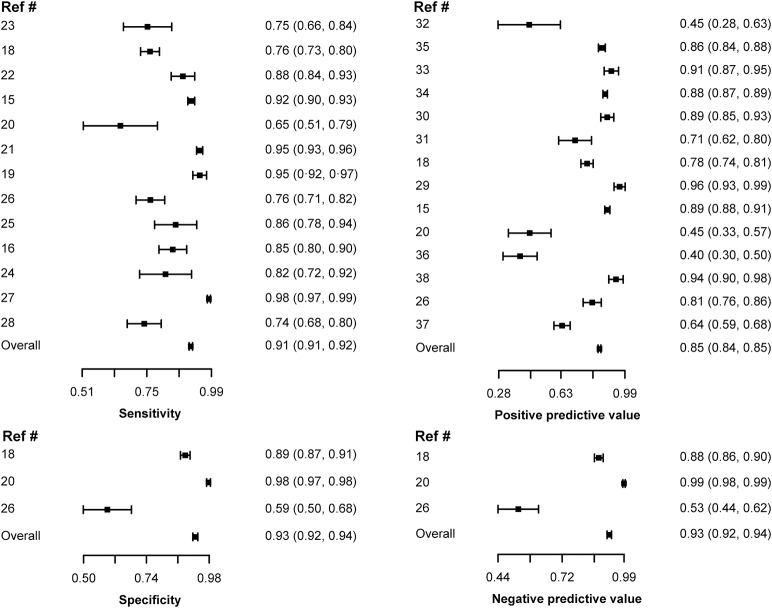
Results: Included studies reported on 15,721 patients. Studies were at low risk of bias. Overall sensitivity (91.3% [95% confidence interval (CI) 90.7-92.0]) and specificity (92.7% [91.7-93.7]) for a cerebrovascular etiology was high, but there was significant variation based on clinical presentation. Misdiagnosis was more frequent among subgroups with milder (SAH with normal vs abnormal mental state; false-negative rate 23.8% vs 4.2%, odds ratio [OR] 7.03 [4.80-10.31]), nonspecific (dizziness vs motor findings; false-negative rate 39.4% vs 4.4%, OR 14.22 [9.76-20.74]), or transient (TIA vs ischemic stroke; false discovery rate 59.7% vs 11.7%, OR 11.21 [6.66-18.89]) symptoms.
Conclusions: Roughly 9% of cerebrovascular events are missed at initial ED presentation. Risk of misdiagnosis is much greater when presenting neurologic complaints are mild, nonspecific, or transient (range 24%-60%). This difference suggests that many misdiagnoses relate to symptom-specific factors. Future research should emphasize studying causes and designing error-reduction strategies in symptom-specific subgroups at greatest risk of misdiagnosis.
© 2017 American Academy of Neurology.
Figures
Comment in
-
Diagnostic errors in cerebrovascular disease: What are we missing?Neurology. 2017 Apr 11;88(15):1390-1391. doi: 10.1212/WNL.0000000000003824. Epub 2017 Mar 29. Neurology. 2017. PMID: 28356462 No abstract available.
References
-
- National Academies of Sciences Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press; 2015.
-
- Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II. N Engl J Med 1991;324:377–384. - PubMed
-
- Saber Tehrani AS, Lee H, Mathews SC, et al. 25-year summary of US malpractice claims for diagnostic errors 1986–2010: an analysis from the National Practitioner Data Bank. BMJ Qual Saf 2013;22:672–680. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical