

Antenatal diagnostic aspects of placenta percreta and its influence on the perinatal outcome: a clinical case and literature review
- PMID: 28356812
- PMCID: PMC5287996
- DOI: 10.6001/actamedica.v23i4.3423
Antenatal diagnostic aspects of placenta percreta and its influence on the perinatal outcome: a clinical case and literature review
Abstract
Background: Placenta percreta is a very rare, but extremely life-threatening obstetrical pathology for the mother and the child, especially in the cases when it is not diagnosed before the birth and when it results in massive bleeding and a dramatic deterioration of condition. It is extremely important to diagnose this pathology as early as possible and plan further optimal care of patients in order to minimize life-threatening complications.
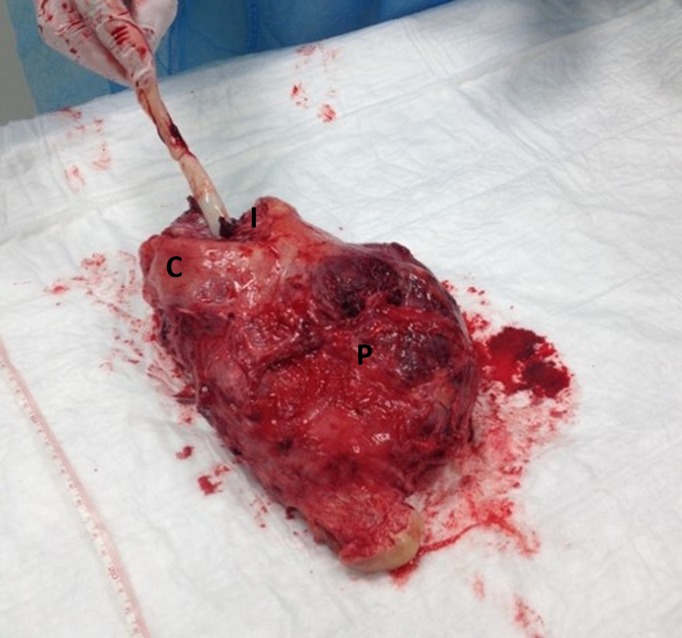
Case report: The paper presents an illustrated clinical case of placenta percreta determined before the birth. Features of visual diagnostics are discussed. A 32-year-old pregnant woman with a history of two caesarean deliveries arrived at the tertiary level hospital at 22 weeks of gestation due to abdomen pain. Placenta previa was diagnosed and ultrasound, magnetic resonance imaging suggesting placenta percreta were seen. On the 32nd week, the planned caesarean hysterectomy was performed. The balloon catheters to occlude the internal iliac arteries and minimize bleeding during the surgery were used.
Conclusions: Antenatal diagnosis of placenta percreta is especially important. Methods of visual diagnostics are complementary. The optimal surgical approach during caesarean hysterectomy remains controversial. In the case of the slow oozing without a clearly identified source of bleeding after hysterectomy and internal iliac arteries balloons deflation, ligation of one of the internal iliac arteriescan be reasonable to avoid residual haemorrhage and relaparotomy.
Santrauka Tikslas. Placentos peraugimas yra labai reta, tačiau motinos ir vaiko sveikatai bei gyvybei pavojinga akušerinė patologija, ypač tais atvejais, kai ji nediagnozuota iki gimdymo ir pasireiškia gausiu kraujavimu bei būklės pablogėjimu. Optimaliai pacientės priežiūrai labai svarbi ankstyva perinatalinė šios patologijos diagnostika. Klinikinis atvejis. Straipsnyje pristatytas iliustruotas peraugusios placentos, nustatytos iki gimdymo, klinikinis atvejis. Aptarti vaizdinės diagnostikos ypatumai. 32 metų nėščioji atvyko į Vilniaus universiteto ligoninės Santariškių klinikas dėl duriančio pobūdžio skausmo pilve. Nėštumo trukmė – 22 savaitės. Moteriai jau buvo atliktos 2 cezario pjūvio operacijos. Ultragarsiniu tyrimu nustatyta placentos pirmeiga, įtartas jos peraugimas. Diagnozei patikslinti atliktas dubens organų magnetinio rezonanso tyrimas ir cistoskopija. Planinis cezario pjūvis atliktas 32 nėštumo savaitę. Dėl galimo intensyvaus kraujavimo operacijos metu į abi vidines klubines arterijas įvesti preokliuziniai balionėliai, kurie užpildyti po naujagimio gimimo. Išvados. Antenatalinė peraugusios placentos diagnostika yra ypač svarbi. Vaizdinės diagnostikos metodai gali papildyti vienas kitą. Optimalus operacijos mastas išlieka kontraversiškas. Raktažodžiai: antenatalinė diagnostika, vaizdinė diagnostika, peraugusi placenta, placentos pirmeiga.
Santrauka Tikslas. Placentos peraugimas yra labai reta, tačiau motinos ir vaiko sveikatai bei gyvybei pavojinga akušerinė patologija, ypač tais atvejais, kai ji nediagnozuota iki gimdymo ir pasireiškia gausiu kraujavimu bei būklės pablogėjimu. Optimaliai pacientės priežiūrai labai svarbi ankstyva perinatalinė šios patologijos diagnostika. Klinikinis atvejis. Straipsnyje pristatytas iliustruotas peraugusios placentos, nustatytos iki gimdymo, klinikinis atvejis. Aptarti vaizdinės diagnostikos ypatumai. 32 metų nėščioji atvyko į Vilniaus universiteto ligoninės Santariškių klinikas dėl duriančio pobūdžio skausmo pilve. Nėštumo trukmė – 22 savaitės. Moteriai jau buvo atliktos 2 cezario pjūvio operacijos. Ultragarsiniu tyrimu nustatyta placentos pirmeiga, įtartas jos peraugimas. Diagnozei patikslinti atliktas dubens organų magnetinio rezonanso tyrimas ir cistoskopija. Planinis cezario pjūvis atliktas 32 nėštumo savaitę. Dėl galimo intensyvaus kraujavimo operacijos metu į abi vidines klubines arterijas įvesti preokliuziniai balionėliai, kurie užpildyti po naujagimio gimimo. Išvados. Antenatalinė peraugusios placentos diagnostika yra ypač svarbi. Vaizdinės diagnostikos metodai gali papildyti vienas kitą. Optimalus operacijos mastas išlieka kontraversiškas. Raktažodžiai: antenatalinė diagnostika, vaizdinė diagnostika, peraugusi placenta, placentos pirmeiga.
Keywords: antenatal diagnostics; placenta percreta; placenta previa; visual diagnostics.
Figures






Similar articles
-
External iliac artery thrombosis after hypogastric artery ligation and pelvic packing for placenta previa percreta.Turk J Obstet Gynecol. 2018 Jun;15(2):130-132. doi: 10.4274/tjod.82642. Epub 2018 Jun 21. Turk J Obstet Gynecol. 2018. PMID: 29971191 Free PMC article.
-
Management of peripartum hysterectomies performed on patients with placenta percreta in a tertiary central hospital.J Matern Fetal Neonatal Med. 2019 Mar;32(6):883-888. doi: 10.1080/14767058.2017.1394289. Epub 2017 Nov 2. J Matern Fetal Neonatal Med. 2019. PMID: 29096564
-
Massive obstetric haemorrhage on post caesarean subtotal hysterectomy due to late detection of occult placenta percreta: A case report.Int J Surg Case Rep. 2021 Aug;85:106225. doi: 10.1016/j.ijscr.2021.106225. Epub 2021 Jul 22. Int J Surg Case Rep. 2021. PMID: 34311343 Free PMC article.
-
Vascular balloon occlusion and planned caesarean hysterectomy for morbidly adherent placenta: A systematic review.Aust N Z J Obstet Gynaecol. 2019 Oct;59(5):608-615. doi: 10.1111/ajo.13027. Epub 2019 Jul 7. Aust N Z J Obstet Gynaecol. 2019. PMID: 31281966
-
Placenta percreta with bladder invasion as a cause of life threatening hemorrhage.J Urol. 2000 Oct;164(4):1270-4. J Urol. 2000. PMID: 10992378 Review.
Cited by
-
Placenta Praevia with Abnormal Adhesion-A Retrospective Study.Clin Pract. 2025 Jan 23;15(2):23. doi: 10.3390/clinpract15020023. Clin Pract. 2025. PMID: 39996693 Free PMC article.
References
-
- Berkley EM, Abuhamad AZ. Prenatal Diagnosis of Placenta Accreta Is Sonography All We Need? Ultrasound Med 2013; 32: 1345–50. - PubMed
-
- Placenta accreta. Committee Opinion No. 529. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012; 120: 207–11. - PubMed
-
- Zlatnik MG, Cheng YW, Norton ME, Thiet MP, Caughey AB. Placenta previa and the risk of preterm delivery. J Matern Fetal Neonatal Med 2007; 20: 719–23. - PubMed
-
- Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, et al. Maternal morbidity associated with multiple repeat cesarean deliveries. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Obstet Gynecol. 2006; 107: 1226–32. - PubMed
-
- Comstock CH. Antenatal diagnosis of placenta accreta: a review. Ultrasound Obstet Gynecol 2005; 26: 89–96. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources