

Refractory burning mouth syndrome: clinical and paraclinical evaluation, comorbiities, treatment and outcome
- PMID: 28357703
- PMCID: PMC5371535
- DOI: 10.1186/s10194-017-0745-y
Refractory burning mouth syndrome: clinical and paraclinical evaluation, comorbiities, treatment and outcome
Abstract
Background: Burning Mouth Syndrome (BMS) is a chronic pain condition characterized by persistent intraoral burning without related objective findings and unknown etiology that affects elderly females mostly. There is no satisfactory treatment for BMS. We aimed to observe the long-term efficacy of high velanfaxine doses combined with systemic and topical administered clonazepam in a particular subgroup of BMS patients who do not respond to current clinical management.
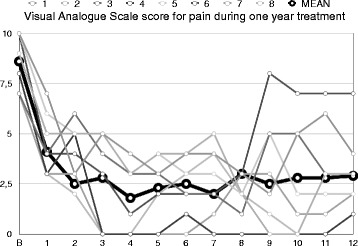
Results: Eight (66.1 ± 6.2 years old females) out of 14 BMS patients fulfilled the inclusion criteria and were treated with venlafaxine (300 mg/d) and clonazepam (5 mg/d) for 35.4 ± 12.1 (mean ± SD) months. The average duration of the symptoms at baseline was 4.3 ± 1.4 years and the overall mean daily pain intensity score was 8.6 ± 1.3 (VAS); pain was in tongue and within the oral mucosa, accompanying by oral and facial dysesthesia. In five patients tasting was abnormal. All patients had positive history of concomitant primary headache. The average score of Hamilton Rating scale for Anxiety and Depression was 21 ± 4.2, and 26.1 ± 2.9, respectively. Previous ineffective treatments include anticonvulsants and anti-depressants. All patients responded (more than 50% decrease in VAS) after three months treatment (mean VAS 3.2 ± 2.2) with no remarkable adverse events.
Conclusion: BMS deserves bottomless psychiatric evaluation and management when current available treatments fail. Treatment with venlafaxine combined with topical and systemic clonazepam may be effective in refractory BMS cases but further investigation in a large-scale controlled study is needed to confirm these results.
Keywords: Burning mouth syndrome; Clinical picture; Clonazepam; Outcome; Treatment; Venlafaxine.
Figures
Similar articles
-
Topical clonazepam for burning mouth syndrome: Is it efficacious in patients with anxiety or depression?J Oral Rehabil. 2022 Jan;49(1):54-61. doi: 10.1111/joor.13275. Epub 2021 Nov 12. J Oral Rehabil. 2022. PMID: 34716948
-
Impact of criteria-based diagnosis of burning mouth syndrome on treatment outcome.J Orofac Pain. 2002 Fall;16(4):305-11. J Orofac Pain. 2002. PMID: 12455431 Clinical Trial.
-
A randomized pilot study to assess the safety and the value of low-level laser therapy versus clonazepam in patients with burning mouth syndrome.Lasers Med Sci. 2016 May;31(4):811-6. doi: 10.1007/s10103-016-1897-8. Epub 2016 Feb 12. Lasers Med Sci. 2016. PMID: 26873501 Clinical Trial.
-
Pharmacological and non-pharmacological management of burning mouth syndrome: A systematic review.Dent Med Probl. 2020 Jul-Sep;57(3):295-304. doi: 10.17219/dmp/120991. Dent Med Probl. 2020. PMID: 33113291
-
Evaluation of the efficacy of treatment modalities in burning mouth syndrome-A systematic review.J Oral Rehabil. 2020 Nov;47(11):1435-1447. doi: 10.1111/joor.13102. Epub 2020 Oct 6. J Oral Rehabil. 2020. PMID: 32979878
Cited by
-
Salivary characteristics may be associated with burning mouth syndrome?J Clin Exp Dent. 2021 Jun 1;13(6):e542-e548. doi: 10.4317/jced.58033. eCollection 2021 Jun. J Clin Exp Dent. 2021. PMID: 34188758 Free PMC article.
-
Psychologic Impact of Chronic Orofacial Pain: A Critical Review.J Oral Facial Pain Headache. 2022 Spring;36(2):103-140. doi: 10.11607/ofph.3010. J Oral Facial Pain Headache. 2022. PMID: 35943323 Free PMC article. Review.
-
Encountering Chronic Sore Throat: How Challenging is it for the Otolaryngologists?Indian J Otolaryngol Head Neck Surg. 2019 Oct;71(Suppl 1):176-181. doi: 10.1007/s12070-017-1191-5. Epub 2017 Sep 6. Indian J Otolaryngol Head Neck Surg. 2019. PMID: 31741956 Free PMC article.
-
Is Burning Mouth Syndrome Associated with Extraoral Dryness? A Systematic Review.J Clin Med. 2023 Oct 14;12(20):6525. doi: 10.3390/jcm12206525. J Clin Med. 2023. PMID: 37892662 Free PMC article. Review.
-
Current management strategies for the pain of elderly patients with burning mouth syndrome: a critical review.Biopsychosoc Med. 2019 Jan 31;13:1. doi: 10.1186/s13030-019-0142-7. eCollection 2019. Biopsychosoc Med. 2019. PMID: 30733824 Free PMC article. Review.
References
-
- Headache Classification Committee of the International Headache Society (IHS). International Classification of Headache Disorders, 3rd edition. Cephalalgia 2013;33:629-808. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
