

ECG-derived spatial QRS-T angle is associated with ICD implantation, mortality and heart failure admissions in patients with LV systolic dysfunction
- PMID: 28358801
- PMCID: PMC5373522
- DOI: 10.1371/journal.pone.0171069
ECG-derived spatial QRS-T angle is associated with ICD implantation, mortality and heart failure admissions in patients with LV systolic dysfunction
Abstract
Background: Increased spatial QRS-T angle has been shown to predict appropriate implantable cardioverter defibrilIator (ICD) therapy in patients with left ventricular systolic dysfunction (LVSD). We performed a retrospective cohort study in patients with left ventricular ejection fraction (LVEF) 31-40% to assess the relationship between the spatial QRS-T angle and other advanced ECG (A-ECG) as well as echocardiographic metadata, with all-cause mortality or ICD implantation for secondary prevention.
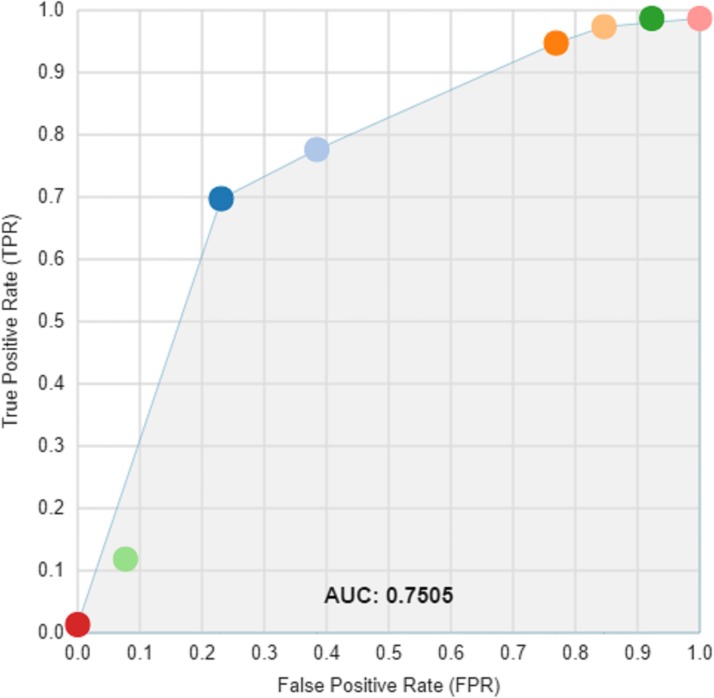
Methods: 534 patients ≤75 years of age with LVEF 31-40% were identified through an echocardiography reporting database. Digital 12-lead ECGs were retrospectively matched to 295 of these patients, for whom echocardiographic and A-ECG metadata were then generated. Data mining was applied to discover novel ECG and echocardiographic markers of risk. Machine learning was used to develop a model to predict possible outcomes.
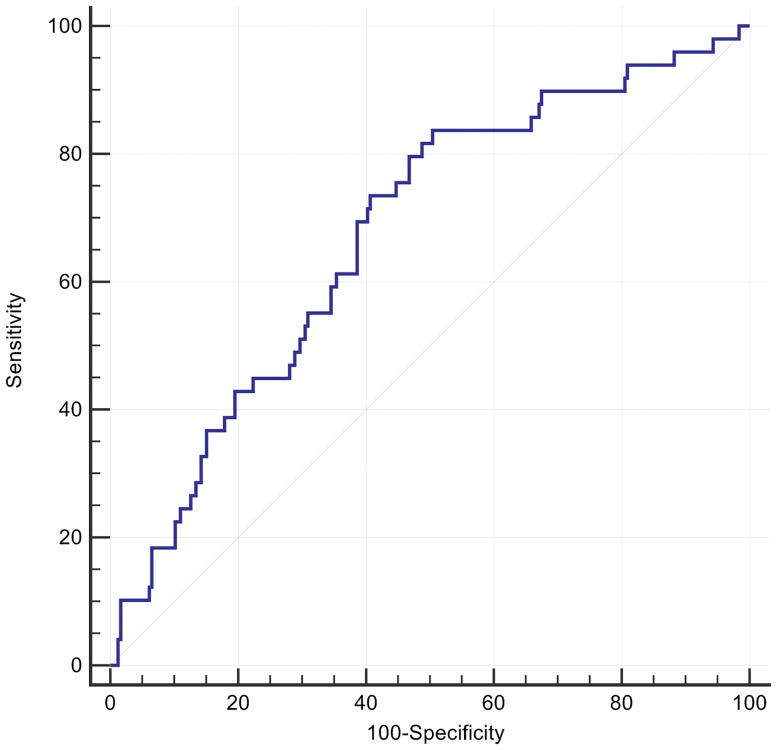
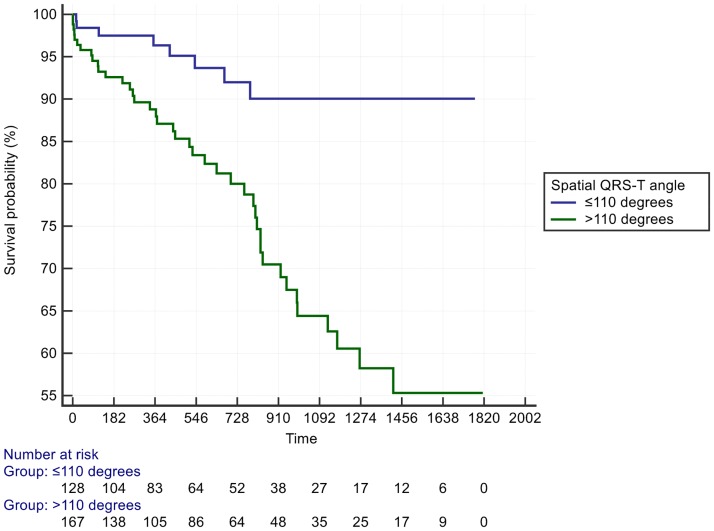
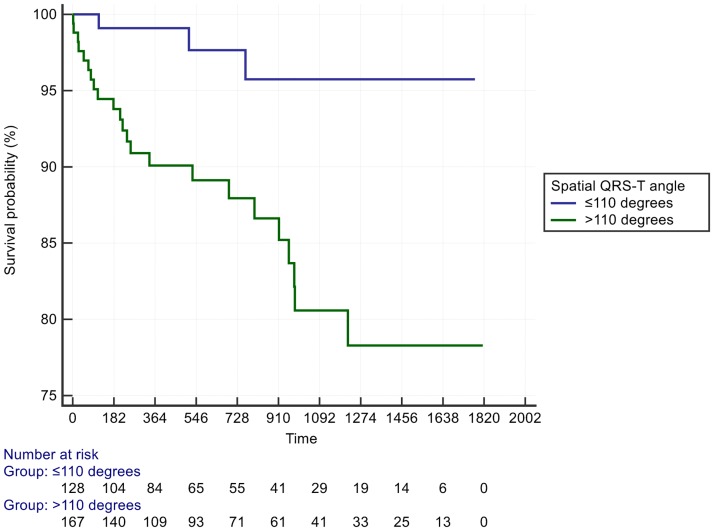
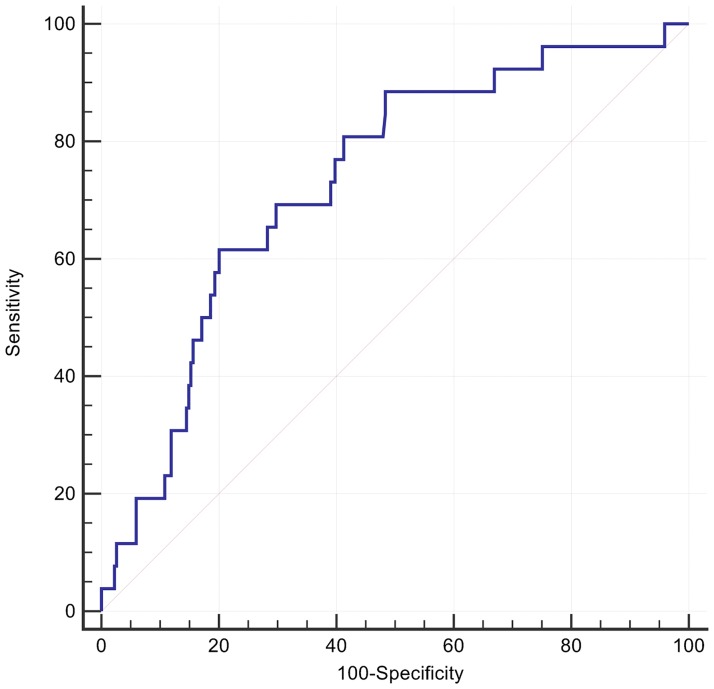
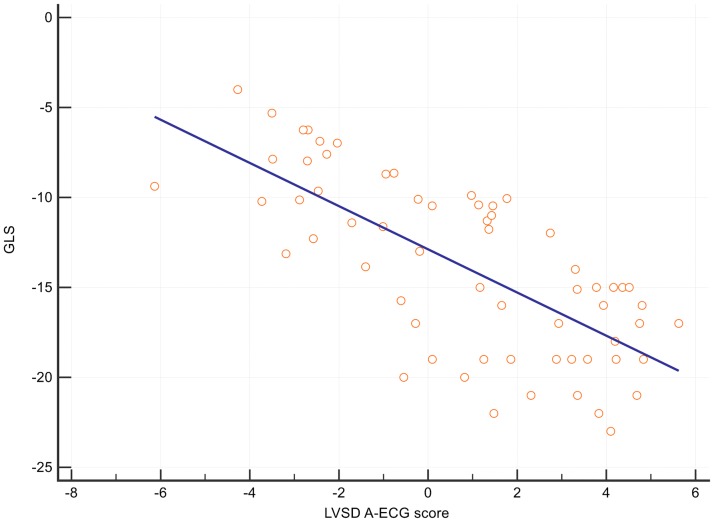
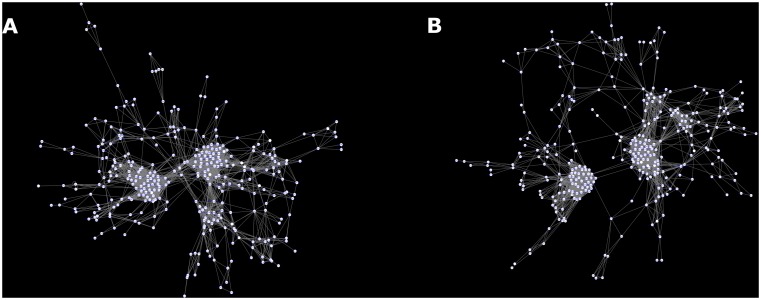
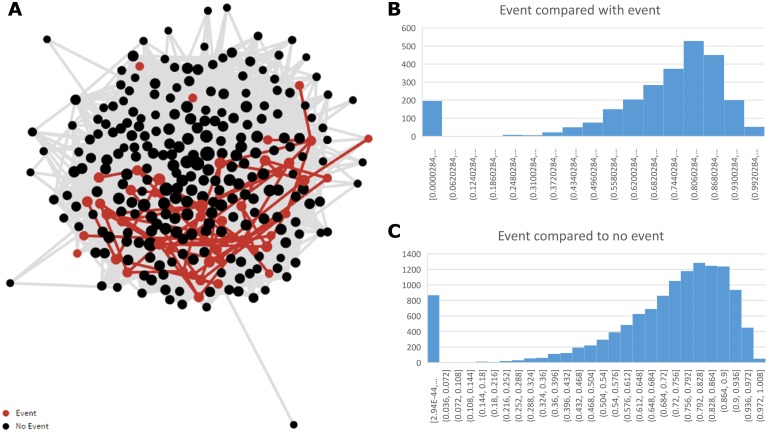
Results: 49 patients (17%) had events, defined as either mortality (n = 16) or ICD implantation for secondary prevention (n = 33). 72 parameters (58 A-ECG, 14 echocardiographic) were univariately different (p<0.05) in those with vs. without events. After adjustment for multiplicity, 24 A-ECG parameters and 3 echocardiographic parameters remained different (p<2x10-3). These included the posterior-to-leftward QRS loop ratio from the derived vectorcardiographic horizontal plane (previously associated with pulmonary artery pressure, p = 2x10-6); spatial mean QRS-T angle (134 vs. 112°, p = 1.6x10-4); various repolarisation vectors; and a previously described 5-parameter A-ECG score for LVSD (p = 4x10-6) that also correlated with echocardiographic global longitudinal strain (R2 = - 0.51, P < 0.0001). A spatial QRS-T angle >110° had an adjusted HR of 3.4 (95% CI 1.6 to 7.4) for secondary ICD implantation or all-cause death and adjusted HR of 4.1 (95% CI 1.2 to 13.9) for future heart failure admission. There was a loss of complexity between A-ECG and echocardiographic variables with an increasing degree of disease.
Conclusion: Spatial QRS-T angle >110° was strongly associated with arrhythmic events and all-cause death. Deep analysis of global ECG and echocardiographic metadata revealed underlying relationships, which otherwise would not have been appreciated. Delivered at scale such techniques may prove useful in clinical decision making in the future.
Conflict of interest statement
Figures
References
-
- Kusumoto FM, Calkins H, Boehmer J, Buxton AE, Chung MK, Gold MR, et al. HRS/ACC/AHA Expert Consensus Statement on the Use of Implantable Cardioverter-Defibrillator Therapy in Patients Who Are Not Included or Not Well Represented in Clinical Trials. Circulation. 2014;130(1):94–125. 10.1161/CIR.0000000000000056 - DOI - PubMed
-
- Kober L, Thune JJ, Nielsen JC, Haarbo J, Videbaek L, Korup E, et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016. Epub 2016/08/30. - PubMed
-
- La Rovere MT, Pinna GD, Maestri R, Mortara A, Capomolla S, Febo O, et al. Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation. 2003;107(4):565–70. Epub 2003/02/05. - PubMed
-
- Piccirillo G, Magri D, Matera S, Magnanti M, Torrini A, Pasquazzi E, et al. QT variability strongly predicts sudden cardiac death in asymptomatic subjects with mild or moderate left ventricular systolic dysfunction: a prospective study. Eur Heart J. 2007;28(11):1344–50. 10.1093/eurheartj/ehl367 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
