

Interventions to treat mental disorders during pregnancy: A systematic review and multiple treatment meta-analysis
- PMID: 28358808
- PMCID: PMC5373816
- DOI: 10.1371/journal.pone.0173397
Interventions to treat mental disorders during pregnancy: A systematic review and multiple treatment meta-analysis
Abstract
Background: For women suffering from an antepartum mental disorder (AMD), there is lack of evidence-based treatment algorithms due to the complicated risk-benefit analysis for both mother and unborn child. We aimed to provide a comprehensive overview of pharmacological and non-pharmacological interventions to treat AMD and performed a meta-analysis of the estimated treatment effect on the psychiatric symptoms during pregnancy.
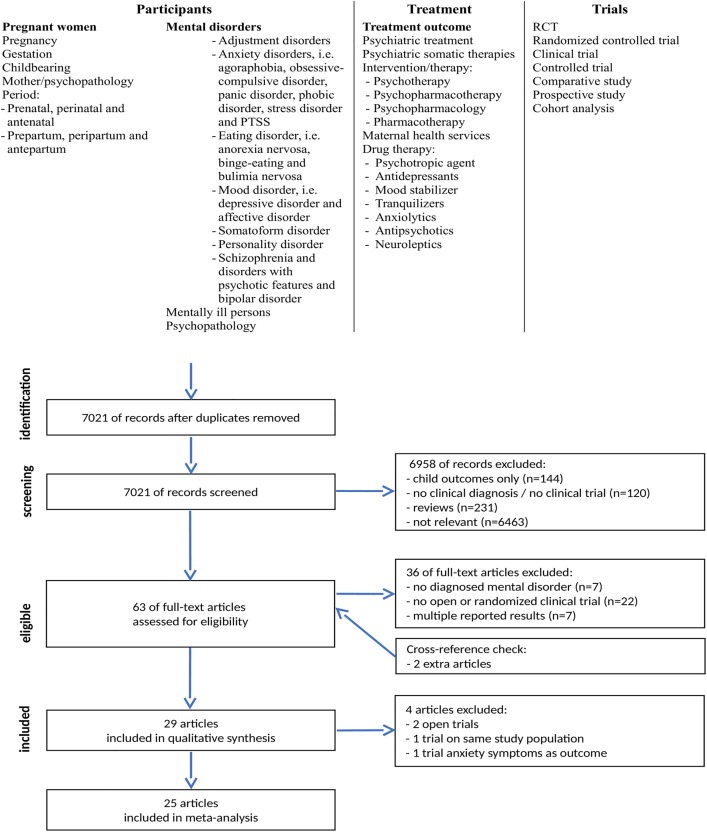
Methods: MedLine, PsycINFO and Embase databases were searched by two independent reviewers for clinical trials with a control condition on treatment of women with AMD, i.e. major depressive (MDD), anxiety, psychotic, eating, somatoform and personality disorders. We inventoried the effect of the treatment, i.e. decrease of psychiatric symptoms at the end of the treatment or postpartum. We adhered to the PRISMA-protocol.
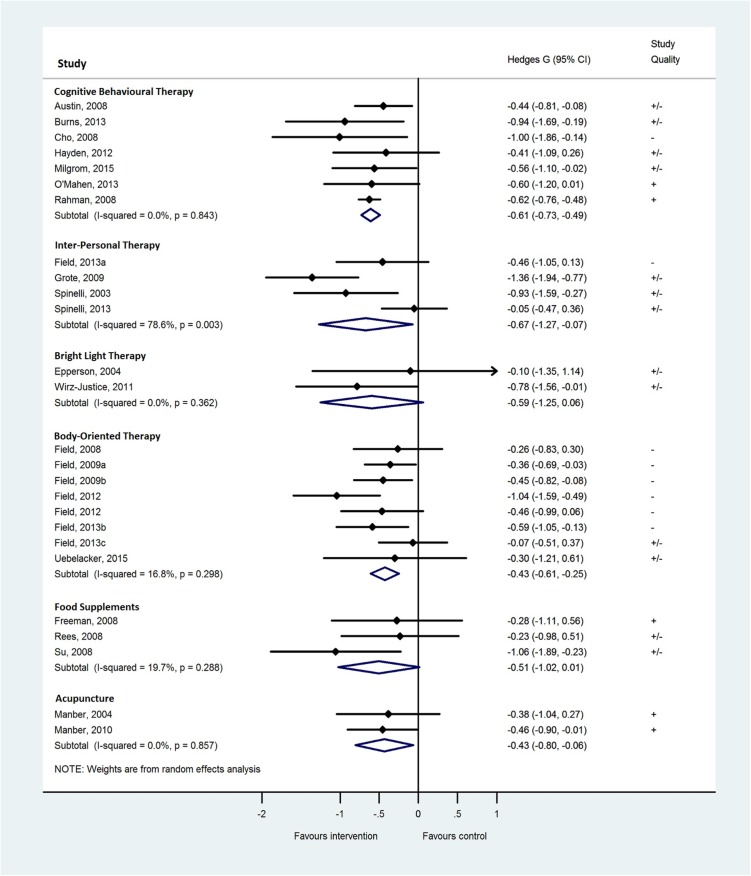
Findings: Twenty-nine trials were found involving 2779 patients. Trials studied patients with depressive disorders (k = 28), and anxiety disorders (k = 1). No pharmacological trials were detected. A form of psychotherapy, like Cognitive Behavioural Therapy (g = -0.61; 95%CI:-0.73 to -0.49, I2 = 0%; k = 7) or Interpersonal Psychotherapy (g = -0.67; 95%CI:-1.27 to -0.07; I2 = 79%; k = 4), holds robust benefit for pregnant women with MDD. Body-oriented interventions (g = -0.43; 95%CI:-0.61 to -0.25; I2 = 17%; k = 7) and acupuncture (g = -0.43; 95%CI:-0.80 to -0.06; I2 = 0%; k = 2) showed medium sized reduction of depressive symptoms. Bright light therapy (g = -0.59; 95%CI:-1.25 to 0.06; I2 = 0%; k = 2), and food supplements (g = -0.51; 95%CI:-1.02 to 0.01; I2 = 20%; k = 3) did not show significant treatment effects. One study was found on Integrative Collaborative Care.
Conclusions: This meta-analysis found a robust moderate treatment effect of CBT for MDD during pregnancy, and to a lesser extent for IPT. As an alternative, positive results were found for body-oriented interventions and acupuncture. No evidence was found for bright light therapy and food supplements. Only non-pharmacological trials on women with MDD were found. Research on a wider range of AMD is needed.
Conflict of interest statement
Figures
References
-
- Bonari L, Pinto N, Ahn E, Einarson A, Steiner M, Koren G. Perinatal Risks of Untreated Depression During Pregnancy. The Canadian Journal of Psychiatry / La Revue canadienne de psychiatrie. 2005;49(11):726–35. - PubMed
-
- Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Depression during pregnancy: Overview of clinical factors. Clin Drug Invest. 2004;24(3):157–79. - PubMed
-
- Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 2005;106(5 Pt 1):1071–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
