

Frequency and clinical significance of short cervix in patients with preterm premature rupture of membranes
- PMID: 28358839
- PMCID: PMC5373606
- DOI: 10.1371/journal.pone.0174657
Frequency and clinical significance of short cervix in patients with preterm premature rupture of membranes
Abstract
Objective: Cervical length measurement has been uggested as a useful tool for predicting intra-amniotic infection/inflammation in preterm labor, but little information is available in the setting of preterm premature rupture of membranes (pPROM). We aimed to determine whether a short cervical length is independently associated with an increased risk of intra-amniotic infection or inflammation and impending preterm delivery in women with pPROM.
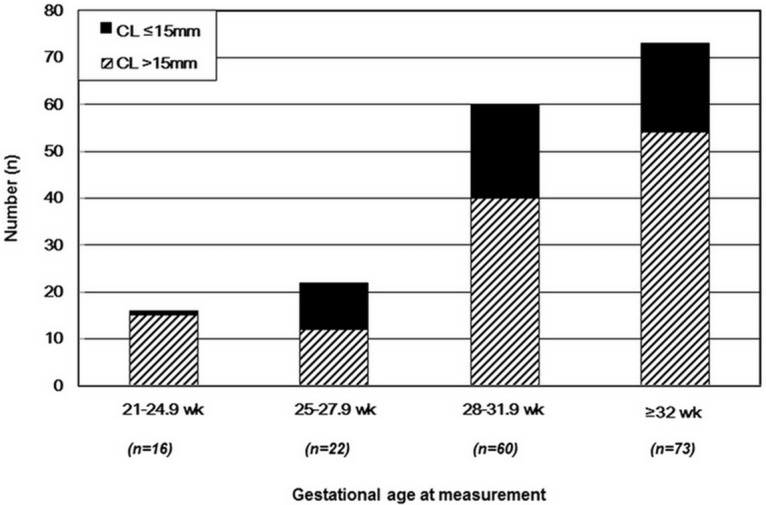
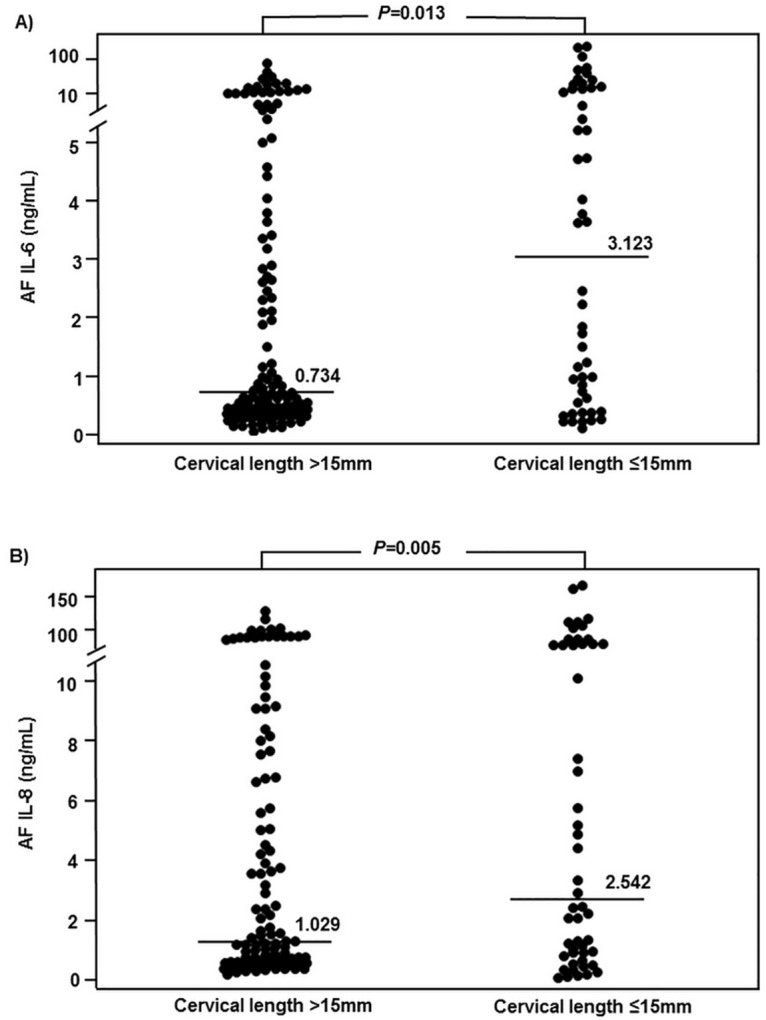
Methods: This was a retrospective cohort study involving 171 consecutive singleton pregnant women with pPROM (21+0-33+6 weeks' gestation), who underwent amniocentesis. Amniotic fluid (AF) was cultured, and assayed for interleukin (IL)-6 and IL-8. Cervical length was measured at the time of amniocentesis by transvaginal ultrasonography with an aseptic technique. Short cervical length was defined as a cervical length of ≤15 mm. Intra-amniotic infection was defined as a positive AF culture for microorganisms and intra-amniotic inflammation was defined as elevated AF concentrations of IL-6 or IL-8 (IL-6 ≥1.5 ng/mL and/or IL-8 ≥1.3 ng/mL).
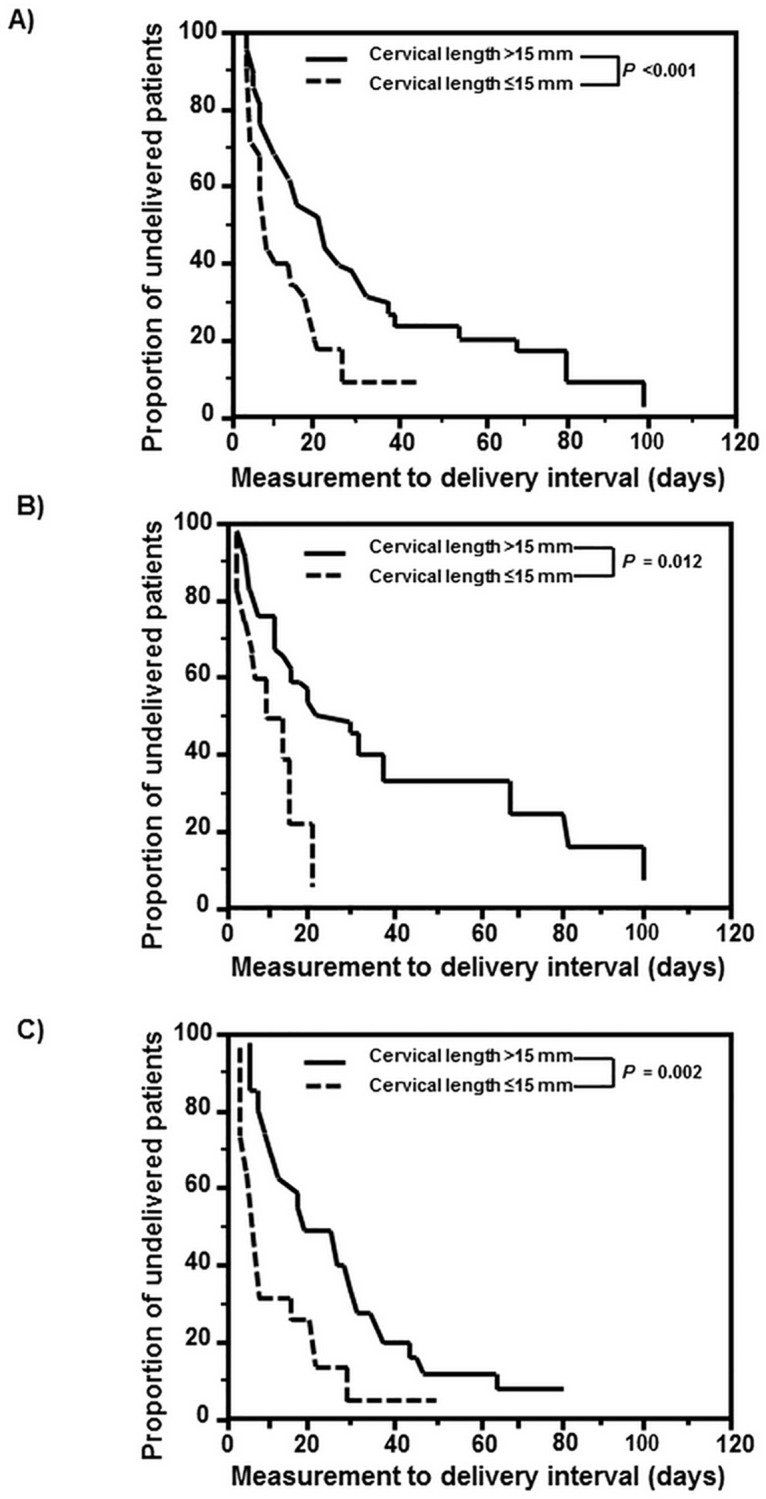
Results: Fifty (29.2%) women had a sonographic cervical length of ≤15mm. On univariate analysis, short cervical length was associated with an increased risk for intra-amniotic infection and/or inflammation; no other parameters studied showed a significant association. Multivariable analyses indicated that short cervical length was significantly associated with a higher risk of impending preterm delivery (within 2 days of measurement, within 7 days of measurement, and before 34 weeks), and remained significant after adjustment for potential confounders.
Conclusion: In women with pPROM, short cervical length is associated with an increased risk for intra-amniotic infection/inflammation and associated with impending preterm delivery, independent of the presence of intra-amniotic infection/inflammation.
Conflict of interest statement
Figures
Similar articles
-
Plasma inflammatory and immune proteins as predictors of intra-amniotic infection and spontaneous preterm delivery in women with preterm labor: a retrospective study.BMC Pregnancy Childbirth. 2018 May 9;18(1):146. doi: 10.1186/s12884-018-1780-7. BMC Pregnancy Childbirth. 2018. PMID: 29743041 Free PMC article.
-
Non-invasive prediction of intra-amniotic infection and/or inflammation in patients with cervical insufficiency or an asymptomatic short cervix (≤15 mm).Arch Gynecol Obstet. 2015 Sep;292(3):579-87. doi: 10.1007/s00404-015-3684-3. Epub 2015 Mar 12. Arch Gynecol Obstet. 2015. PMID: 25762201
-
Transvaginal ultrasonographic measurement of cervical length in predicting intra-amniotic infection and impending preterm delivery in preterm labor: a comparison with amniotic fluid white blood cell count.J Perinat Med. 2008;36(6):479-84. doi: 10.1515/JPM.2008.071. J Perinat Med. 2008. PMID: 18651831
-
The prevalence and clinical significance of intraamniotic infection with Candida species in women with preterm labor.Arch Gynecol Obstet. 1992;251(1):9-15. doi: 10.1007/BF02718273. Arch Gynecol Obstet. 1992. PMID: 1550392 Review.
-
The diagnosis of intrauterine infection in women with preterm premature rupture of the membranes (PPROM).Clin Obstet Gynecol. 1998 Dec;41(4):849-63. doi: 10.1097/00003081-199812000-00009. Clin Obstet Gynecol. 1998. PMID: 9917940 Review. No abstract available.
Cited by
-
Determinants of prelabor rupture of membrane among pregnant women attending governmental hospitals in Jimma zone, Oromia region, Ethiopia: A multi-center case-control study.PLoS One. 2023 Nov 30;18(11):e0294482. doi: 10.1371/journal.pone.0294482. eCollection 2023. PLoS One. 2023. PMID: 38033036 Free PMC article.
-
Proteomic analysis of plasma to identify novel biomarkers for intra-amniotic infection and/or inflammation in preterm premature rupture of membranes.Sci Rep. 2023 Apr 6;13(1):5658. doi: 10.1038/s41598-023-32884-y. Sci Rep. 2023. PMID: 37024561 Free PMC article.
-
[Effect of different antibiotic use strategies on infection in neonates with premature rupture of membranes and high-risk factors for neonatal infection].Zhongguo Dang Dai Er Ke Za Zhi. 2020 Apr;22(4):310-315. doi: 10.7499/j.issn.1008-8830.1910170. Zhongguo Dang Dai Er Ke Za Zhi. 2020. PMID: 32312367 Free PMC article. Chinese.
-
A protein microarray analysis of amniotic fluid proteins for the prediction of spontaneous preterm delivery in women with preterm premature rupture of membranes at 23 to 30 weeks of gestation.PLoS One. 2020 Dec 31;15(12):e0244720. doi: 10.1371/journal.pone.0244720. eCollection 2020. PLoS One. 2020. PMID: 33382822 Free PMC article.
-
The impact of cervical conization size with subsequent cervical length changes on preterm birth rates in asymptomatic singleton pregnancies.Sci Rep. 2021 Oct 5;11(1):19703. doi: 10.1038/s41598-021-99185-0. Sci Rep. 2021. PMID: 34611206 Free PMC article.
References
-
- Kaltreider DF, Kohl S. Epidemiology of preterm delivery. Clin Obstet Gynecol. 1980;23(1):17–31. - PubMed
-
- Garite TJ, Freeman RK, Linzey EM, Braly P. The use of amniocentesis in patients with premature rupture of membranes. Obstet Gynecol. 1979;54(2):226–30. - PubMed
-
- Vintzileos AM, Campbell WA, Nochimson DJ, Weinbaum PJ, Escoto DT, Mirochnick MH. Qualitative amniotic fluid volume versus amniocentesis in predicting infection in preterm premature rupture of the membranes. Obstet Gynecol. 1986;67(4):579–83. - PubMed
-
- Gauthier DW, Meyer WJ, Bieniarz A. Correlation of amniotic fluid glucose concentration and intraamniotic infection in patients with preterm labor or premature rupture of membranes. Am J Obstet Gynecol. 1991;165(4 Pt 1):1105–10. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
