

Assessment of the retinal posterior pole in dominant optic atrophy by spectral-domain optical coherence tomography and microperimetry
- PMID: 28358911
- PMCID: PMC5373574
- DOI: 10.1371/journal.pone.0174560
Assessment of the retinal posterior pole in dominant optic atrophy by spectral-domain optical coherence tomography and microperimetry
Abstract
Background: To assess posterior pole (PP) retinal structure in patients with genetically confirmed autosomal dominant optic atrophy (ADOA) using new spectral domain optical coherence tomography (SD-OCT) segmentation technology. To analyze retinal PP thickness in relation to retinal sensitivity data from microperimetry (MP) in ADOA patients.
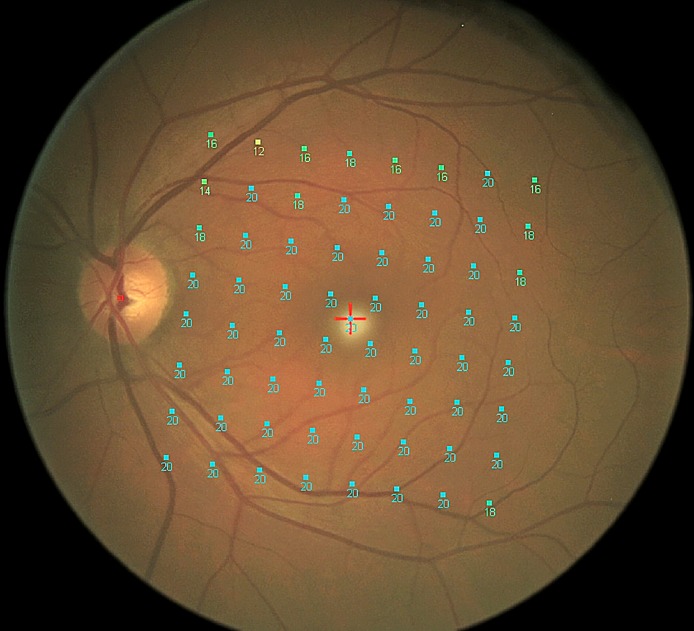
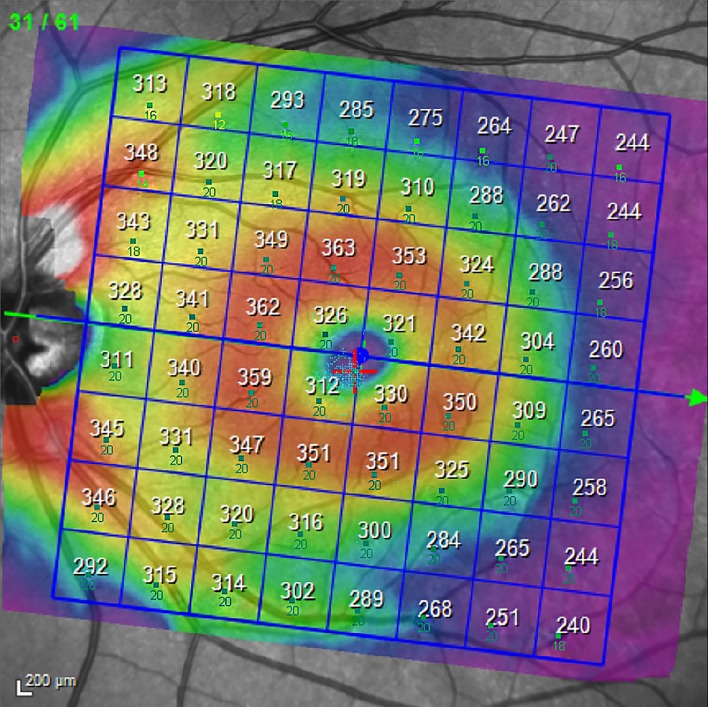
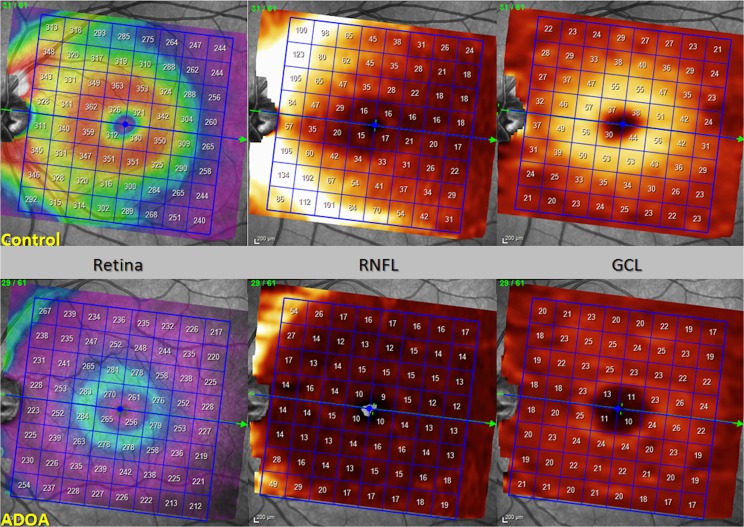
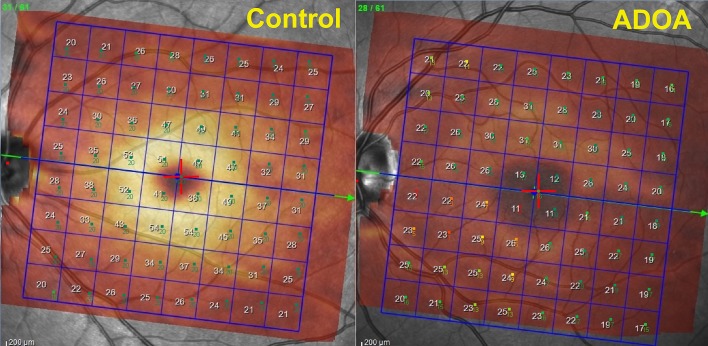
Methods and findings: This prospective cross-sectional study included 11 patients with ADOA and 11 age-matched healthy subjects. All participants underwent both a "Posterior Pole" and "peripapillary RNFL (pRNFL)" scanning protocol using SD-OCT. Functional mapping of the PP was also performed using MP. A customized program was implemented in order to achieve accurate superimposition of MP sensitivity map onto SD-OCT map. The thickness of the PP different retinal layers and pRNFL was obtained and measured for each eye. Mean retinal sensitivity values and fixation stability were obtained and compared between ADOA patients and healthy subjects. Correlation analysis was performed on a point-to-point basis to evaluate the association between mean thickness and retinal sensitivity of each retinal layer. Total retinal thickness (TRT), Retinal Nerve Fiber Layer (RNFL), Ganglion Cell Layer (GCL), Inner Plexiform Layer (IPL), Inner Nuclear Layer (INL) and Inner Retinal Layers (IRL) at the posterior pole as well as pRNFL were significantly thinner in ADOA patients (P < 0.0001). On the contrary, the Outer Plexiform Layer (OPL) and the Outer Nuclear Layer (ONL) were significantly thicker in the ADOA group (P < 0.001). No significant differences were found in Retinal Pigment Epithelium (RPE) and Outer Retinal Layers (ORL) thickness between ADOA and controls. The average PP retinal sensitivity was significantly reduced in ADOA patients compared with controls (P < 0.001), as measured by microperimeter Nidek MP-1 (MP1). Fixation stability was significantly worse in the ADOA group (P = 0.01). The most severe sensitivity defects in ADOA patients were found at the level of the papillo-macular bundle (PMB).
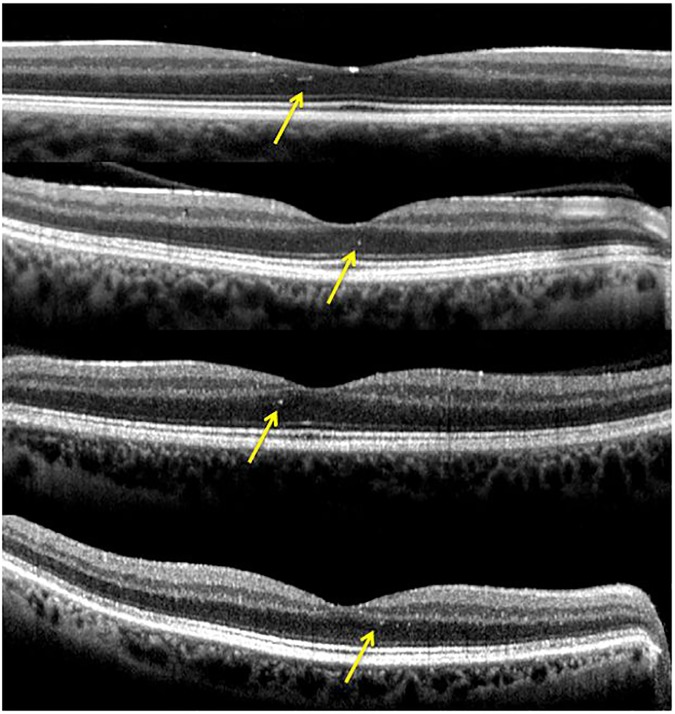
Conclusions: Inner retinal layers showed pathological changes in ADOA patients. In addition, the whole retinal PP (not only the PMB) was significantly altered in ADOA, both in terms of retinal thickness and sensitivity.
Conflict of interest statement
Figures
References
-
- Kjer B, Eiberg H, Kjer P, Rosenberg T. Dominant optic atrophy mapped to chromosome 3q region. II. Clinical and epidemiological aspects. Acta Ophthalmol Scand. 1996;74:3–7. - PubMed
-
- Eliott D, Traboulsi EI, Maumenee IH. Visual prognosis in autosomal dominant optic atrophy (Kjer type). Am J Ophthalmol. 1993;115:360–7. - PubMed
-
- Votruba M, Fitzke FW, Holder GE, Carter A, Bhattacharya SS, Moore AT. Clinical features in affected individuals from 21 pedigrees with dominant optic atrophy. Arch Ophthalmol. 1998;116:351–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
