

Association of Radiotherapy Boost for Ductal Carcinoma In Situ With Local Control After Whole-Breast Radiotherapy
- PMID: 28358936
- PMCID: PMC5824216
- DOI: 10.1001/jamaoncol.2016.6948
Association of Radiotherapy Boost for Ductal Carcinoma In Situ With Local Control After Whole-Breast Radiotherapy
Abstract
Importance: The use of a radiotherapy (RT) boost to the tumor bed after whole-breast RT (WBRT) for ductal carcinoma in situ (DCIS) is largely extrapolated from invasive cancer data, but robust evidence specific to DCIS is lacking.
Objective: To compare ipsilateral breast tumor recurrence (IBTR) in women with DCIS treated with vs without the RT boost after breast-conserving surgery and WBRT.
Design, setting, and participants: This retrospective analysis pooled deidentified patient-level data from 10 academic institutions in the United States, Canada, and France from January 1, 1980, through December 31, 2010. All patients had newly diagnosed pure DCIS (no microinvasion), underwent breast-conserving surgery, and received WBRT with or without the boost with a minimum of 5 years of follow-up required for inclusion in the analysis. Given the limited events after WBRT, an a priori power analysis was conducted to estimate the DCIS sample size needed to detect the anticipated benefit of the boost. Data were uniformly recoded at the host institution and underwent primary and secondary reviews before analysis. Sample size calculations (ratio of patients who received the boost dose to those who did not, 2:1; α = .05; power = 80%) estimated that 2982 cases were needed to detect a difference of at least 3%. The final analysis included 4131 patients (2661 in the boost group and 1470 in the no-boost group) with a median follow-up of 9 years and media boost dose of 14 Gy. Data were collected from July 2011 through February 2014 and analyzed from March 2014 through August 2015.
Interventions: Radiotherapy boost vs no boost.
Main outcomes and measures: Ipsilateral breast tumor recurrence.
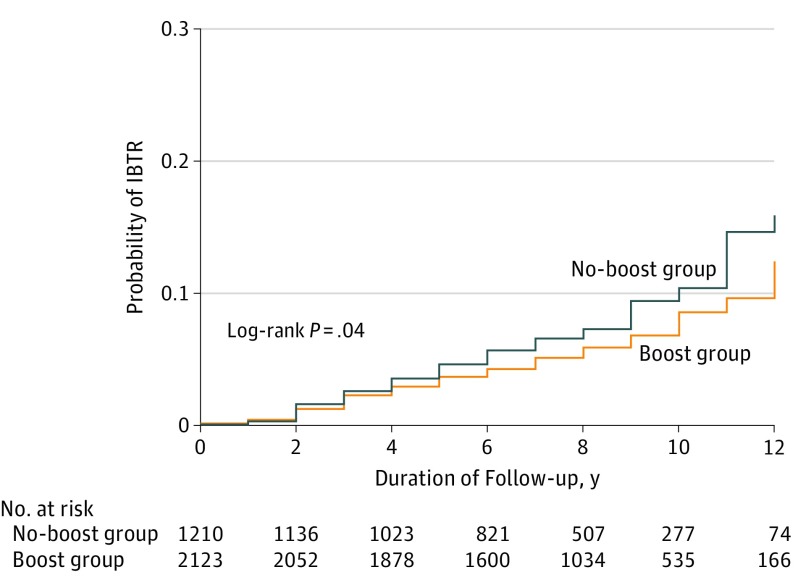
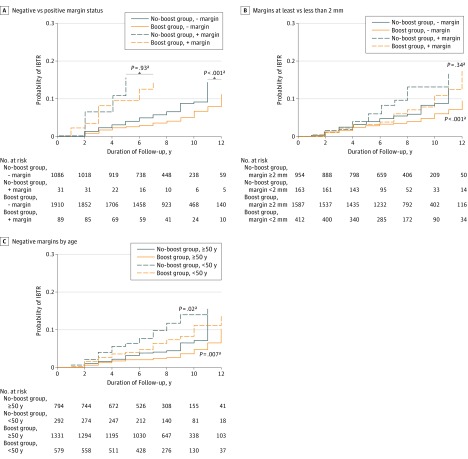
Results: The analysis included 4131 patients (median [SD] age, 56.1 [10.9] years; range, 24-88 years). Patients with positive margins, unknown estrogen receptor status, and comedo necrosis were more likely to have received an RT boost. For the entire cohort, the boost was significantly associated with lower IBTR (hazard ratio [HR], 0.73; 95% CI, 0.57-0.94; P = .01) and with IBTR-free survival (boost vs no-boost groups) of 97.1% (95% CI, 0.96-0.98) vs 96.3% (95% CI, 0.95-0.97) at 5 years, 94.1% (95% CI, 0.93-0.95) vs 92.5% (95% CI, 0.91-0.94) at 10 years, and 91.6% (95% CI, 0.90-0.93) vs 88.0% (95% CI, 0.85-0.91) at 15 years. On multivariable analysis accounting for confounding factors, the boost remained significantly associated with reduced IBTR (HR compared with no boost, 0.68; 95% CI, 0.50-0.91; P = .01) independent of age and tamoxifen citrate use.
Conclusions and relevance: This patient-level analysis suggests that the RT boost confers a statistically significant benefit in decreasing IBTR across all DCIS age groups, similar to that seen in patients with invasive breast cancer. These findings suggest that a DCIS RT boost to the tumor bed could be considered to provide an added incremental benefit in decreasing IBTR after a shared discussion between the patient and her radiation oncologist.
Conflict of interest statement
Figures
References
-
- DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics, 2011. CA Cancer J Clin. 2011;61(6):409-418. - PubMed
-
- Holmberg L, Garmo H, Granstrand B, et al. Absolute risk reductions for local recurrence after postoperative radiotherapy after sector resection for ductal carcinoma in situ of the breast. J Clin Oncol. 2008;26(8):1247-1252. - PubMed
-
- Bijker N, Meijnen P, Peterse JL, et al. ; EORTC Breast Cancer Cooperative Group; EORTC Radiotherapy Group . Breast-conserving treatment with or without radiotherapy in ductal carcinoma-in-situ: ten-year results of European Organisation for Research and Treatment of Cancer randomized phase III trial 10853—a study by the EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. J Clin Oncol. 2006;24(21):3381-3387. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
