

Pelvimetry for fetal cephalic presentations at or near term for deciding on mode of delivery
- PMID: 28358979
- PMCID: PMC6464150
- DOI: 10.1002/14651858.CD000161.pub2
Pelvimetry for fetal cephalic presentations at or near term for deciding on mode of delivery
Abstract
Background: Pelvimetry assesses the size of a woman's pelvis aiming to predict whether she will be able to give birth vaginally or not. This can be done by clinical examination, or by conventional X-rays, computerised tomography (CT) scanning, or magnetic resonance imaging (MRI).
Objectives: To assess the effects of pelvimetry (performed antenatally or intrapartum) on the method of birth, on perinatal mortality and morbidity, and on maternal morbidity. This review concentrates exclusively on women whose fetuses have a cephalic presentation.
Search methods: We searched Cochrane Pregnancy and Childbirth Group's Trials Register (31 January 2017) and reference lists of retrieved studies.
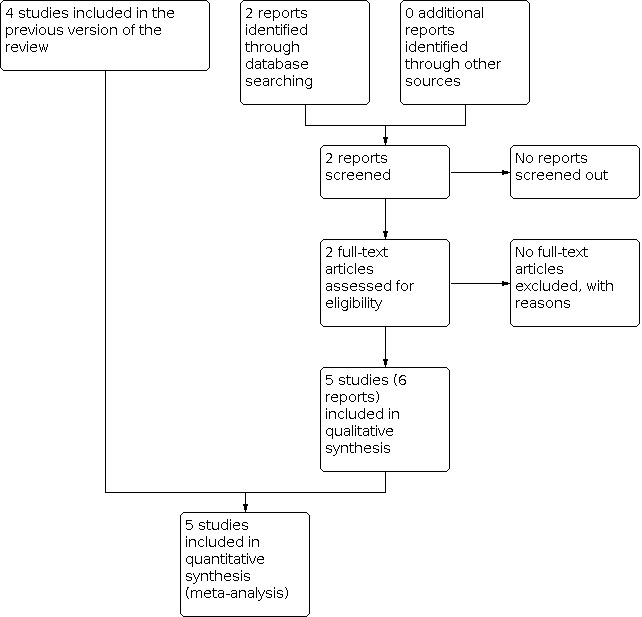
Selection criteria: Randomised controlled trials (including quasi-randomised) assessing the use of pelvimetry versus no pelvimetry or assessing different types of pelvimetry in women with a cephalic presentation at or near term were included. Cluster trials were eligible for inclusion, but none were identified.
Data collection and analysis: Two review authors independently assessed trials for inclusion and risk of bias, extracted data and checked them for accuracy. We assessed the quality of the evidence using the GRADE approach.
Main results: Five trials with a total of 1159 women were included. All used X-ray pelvimetry to assess the pelvis. X-ray pelvimetry versus no pelvimetry or clinical pelvimetry is the only comparison included in this review due to the lack of trials identified that examined other types of radiological pelvimetry or that compared clinical pelvimetry versus no pelvimetry.The included trials were generally at high risk of bias. There is an overall high risk of performance bias due to lack of blinding of women and staff. Two studies were also at high risk of selection bias. We used GRADEpro software to grade evidence for our selected outcomes; for caesarean section we rated the evidence low quality and all the other outcomes (perinatal mortality, wound sepsis, blood transfusion, scar dehiscence and admission to special care baby unit) as very low quality. Downgrading was due to risk of bias relating to lack of allocation concealment and blinding, and imprecision of effect estimates.Women undergoing X-ray pelvimetry were more likely to have a caesarean section (risk ratio (RR) 1.34, 95% confidence interval (CI) 1.19 to 1.52; 1159 women; 5 studies; low-quality evidence). There were no clear differences between groups for perinatal outcomes: perinatal mortality (RR 0.53, 95% CI 0.19 to 1.45; 1159 infants; 5 studies; very low-quality evidence), perinatal asphyxia (RR 0.66, 95% CI 0.39 to 1.10; 305 infants; 1 study), and admission to special care baby unit (RR 0.20, 95% CI 0.01 to 4.13; 288 infants; 1 study; very low-quality evidence). Other outcomes assessed were wound sepsis (RR 0.83, 95% CI 0.26 to 2.67; 288 women; 1 study; very low-quality evidence), blood transfusion (RR 1.00, 95% CI 0.39 to 2.59; 288 women; 1 study; very low-quality evidence), and scar dehiscence (RR 0.59, 95% CI 0.14 to 2.46; 390 women; 2 studies; very low-quality evidence). Again, no clear differences were found for these outcomes between the women who received X-ray pelvimetry and those who did not. Apgar score less than seven at five minutes was not reported in any study.
Authors' conclusions: X-ray pelvimetry versus no pelvimetry or clinical pelvimetry is the only comparison included in this review due to the lack of trials identified that used other types or pelvimetry (other radiological examination or clinical pelvimetry versus no pelvimetry). There is not enough evidence to support the use of X-ray pelvimetry for deciding on mode of delivery in women whose fetuses have a cephalic presentation. Women who undergo an X-ray pelvimetry may be more likely to have a caesarean section.Further research should be directed towards defining whether there are specific clinical situations in which pelvimetry can be shown to be of value. Newer methods of pelvimetry (CT, MRI) should be subjected to randomised trials to assess their value. Further trials of X-ray pelvimetry in cephalic presentations would be of value if large enough to assess the effect on perinatal mortality.
Conflict of interest statement
Robert C Pattinson: no conflict of interest. Anna Cuthbert: no conflict of interest. Valerie Vannevel: no conflict of interest.
Figures










Update of
-
Pelvimetry for fetal cephalic presentations at term.Cochrane Database Syst Rev. 2000;(2):CD000161. doi: 10.1002/14651858.CD000161. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2017 Mar 30;3:CD000161. doi: 10.1002/14651858.CD000161.pub2. PMID: 10796162 Updated.
References
References to studies included in this review
Crichton 1962 {published data only}
-
- Crichton D. The accuracy and value of cephalopelvimetry. Journal of Obstetrics and Gynaecology of the British Commonwealth 1962;69:366-78.
Gaitan 2009 {published data only}
-
- Gaitan N, Duenas JL, Bedoya C, Taboada C, Polo J. Prospective, randomised and controlled study to evaluate the usefulness of radiopelvimetry in induced labour in primigravidae [Estudio prospectivo, aleatorizado y controlado para evaluar la utilidad de la radiopelvimetria en la induccion de parto en primigravidas]. Progresos de Obstetricia y Ginecologia 2009;52(10):552-6.
-
- Gaitan Quintero N, Duenas Diez JL, Bedoya Bergua C, Taboada Montes C, Padillo JP. The use of the radiopelvimetria previously to the induction of labor in primigravidas. Journal of Maternal-Fetal and Neonatal Medicine 2010;23(S1):278.
Parsons 1985 {published data only}
-
- Parsons MT, Spellacy WN. Prospective randomised study of X-ray pelvimetry in the primigravida. Obstetrics & Gynecology 1985;66:76-9. - PubMed
Richards 1985 {published data only}
-
- Richards A, Strang A, Moodley J, Philpott H. Vaginal delivery following caesarean section - is X-ray pelvimetry a reliable predictor? In: Proceedings of 4th Conference on Priorities in Perinatal Care in South Africa, 1985; Natal, South Africa. 1985:62-5.
Thubisi 1993 {published data only}
-
- Thubisi M, Ebrahim A, Moodley J, Shweni PM. Vaginal delivery after previous caesarean section: is X-ray pelvimetry necessary? British Journal of Obstetrics and Gynaecology 1993;100:421-4. - PubMed
References to studies excluded from this review
Farrell 2002 {unpublished data only}
-
- Volschenk S, Farrell E, Jeffery BS, Pattinson RC. Clinical pelvimetry as a predictor of vaginal delivery in women with one previous caesarean section. In: 20th Conference on Priorities in Perinatal Care in Southern Africa; 2001 March 6-9; KwaZulu-Natal, South Africa. 2002.
Additional references
Catling‐Paull 2011
-
- Catling-Paull C, Johnston R, Ryan C, Foureur MJ, Homer CSE. Clinical interventions that increase the uptake and success of vaginal birth after caesarean section: a systematic review. Journal of Advanced Nursing 2011;67(8):1646-61. - PubMed
Dodd 2013
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Mengert 1948
-
- Mengert WF. Estimation of pelvic capacity. JAMA 1948;138:169-74. - PubMed
Morgan 1992
-
- Morgan MA, Thurnau GR. Efficacy of the fetal-pelvic index in nulliparous women at high risk for fetal-pelvic disproportion. American Journal of Obstetrics and Gynecology 1992;166(3):810-4. - PubMed
Morris 1993
-
- Morris CW, Heggie JCP, Acton CM. Computed tomography pelvimetry: accuracy and radiation dose compared with conventional pelvimetry. Australasian Radiology 1993;37:186-91. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sporri 2002
-
- Sporri S, Thoeny HC, Raio L, Lachat R, Vock P, Schneider H. MR imaging pelvimetry: a useful adjunct in the treatment of women at risk for dystocia? American Journal of Roentgenology 2002;179:137-44. - PubMed
van Ham 1997
-
- Ham MAEC, Dongen PWJ, Mulder J. Maternal consequences of caesarean section - A retrospective study of intra-operative and postoperative maternal complications of caesarean section during a 10-year period. European Journal of Obstetrics & Gynecology and Reproductive Biology 1997;74:1-6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical