

High Risk of Seizures and Epilepsy after Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Stroke
- PMID: 28359069
- PMCID: PMC5425760
- DOI: 10.1159/000458730
High Risk of Seizures and Epilepsy after Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Stroke
Abstract
Background: Decompressive hemicraniectomy (DHC) is a life-saving procedure for treatment of large malignant middle cerebral artery (MCA) strokes. Post-stroke epilepsy is an additional burden for these patients, but its incidence and the risk factors for its development have been poorly investigated.
Objective: To report the prevalence and risk factors for post-stroke seizures and post-stroke epilepsy after DHC for treatment of large malignant MCA strokes in a cohort of 36 patients.
Methods: In a retrospective cohort study of 36 patients we report the timing and incidence of post-stroke epilepsy. We analyzed if age, sex, vascular risk factors, side of ischemia, reperfusion therapy, stroke etiology, extension of stroke, hemorrhagic transformation, ECASS scores, National Institutes of Health Stroke Scale (NIHSS) scores, or modified Rankin scores were risk factors for seizure or epilepsy after DHC for treatment of large MCA strokes.
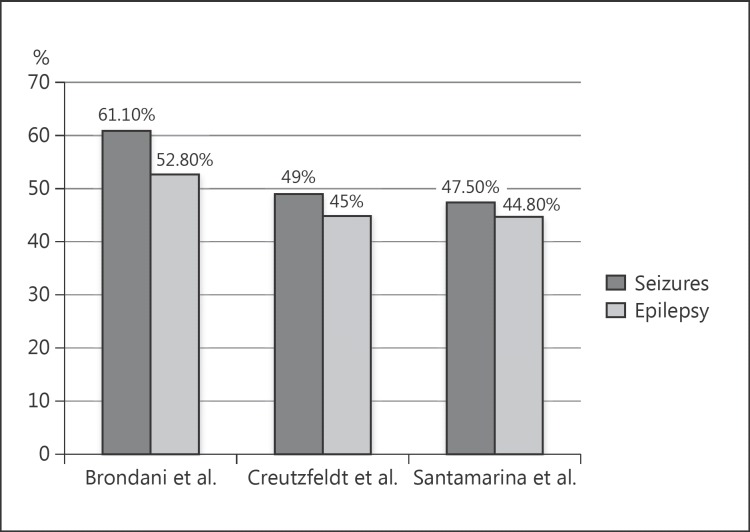
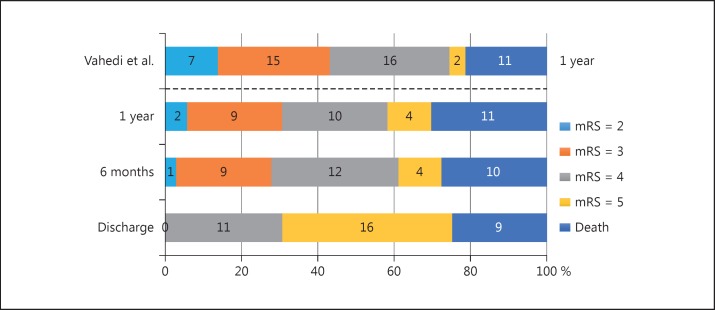
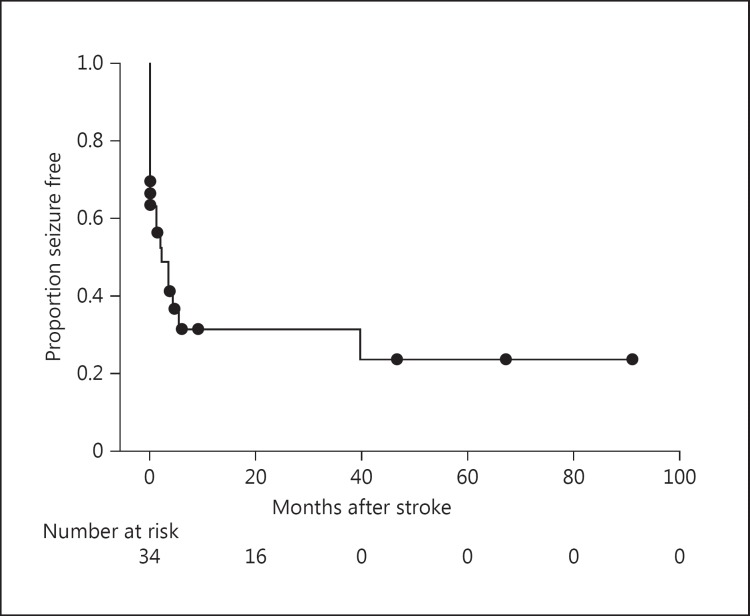
Results: The mean patient follow-up time was 1,086 days (SD = 1,172). Out of 36 patients, 9 (25.0%) died before being discharged. After 1 year, a total of 11 patients (30.6%) had died, but 22 (61.1%) of them had a modified Rankin score ≤4. Thirteen patients (36.1%) developed seizures within the first week after stroke. Seizures occurred in 22 (61.1%) of 36 patients (95% CI = 45.17-77.03%). Out of 34 patients who survived the acute period, 19 (55.9%) developed epilepsy after MCA infarcts and DHC (95% CI = 39.21-72.59%). In this study, no significant differences were observed between the patients who developed seizures or epilepsy and those who remained free of seizures or epilepsy regarding age, sex, side of stroke, presence of the clinical risk factors studied, hemorrhagic transformation, time of craniectomy, and Rankin score after 1 year of stroke.
Conclusion: The incidence of seizures and epilepsy after malignant MCA infarcts submitted to DHC might be very high. Seizure might occur precociously in patients who are not submitted to anticonvulsant prophylaxis. The large stroke volume and the large cortical ischemic area seem to be the main risk factors for seizure or epilepsy development in this subtype of stroke. .
Keywords: Post-stroke epilepsy; Risk factors for epilepsy; Risk factors for seizures; Seizure prophylaxis; Stroke.
© 2017 The Author(s) . Published by S. Karger AG, Basel.
Figures
Similar articles
-
Nationwide survey of decompressive hemicraniectomy for malignant middle cerebral artery infarction in Japan.World Neurosurg. 2014 Dec;82(6):1158-63. doi: 10.1016/j.wneu.2014.07.015. Epub 2014 Jul 18. World Neurosurg. 2014. PMID: 25045787
-
Predictors of In-Hospital Mortality after Decompressive Hemicraniectomy for Malignant Ischemic Stroke.J Stroke Cerebrovasc Dis. 2017 Sep;26(9):1941-1947. doi: 10.1016/j.jstrokecerebrovasdis.2017.06.021. Epub 2017 Jul 8. J Stroke Cerebrovasc Dis. 2017. PMID: 28694110
-
Decompressive hemicraniectomy, strokectomy, or both in the treatment of malignant middle cerebral artery syndrome.World Neurosurg. 2012 Nov;78(5):480-6. doi: 10.1016/j.wneu.2011.12.080. Epub 2011 Dec 24. World Neurosurg. 2012. PMID: 22381279
-
Hemicraniectomy versus medical treatment with large MCA infarct: a review and meta-analysis.BMJ Open. 2016 Nov 24;6(11):e014390. doi: 10.1136/bmjopen-2016-014390. BMJ Open. 2016. PMID: 27884858 Free PMC article. Review.
-
Assessment of outcome following decompressive craniectomy for malignant middle cerebral artery infarction in patients older than 60 years of age.Neurosurg Focus. 2009 Jun;26(6):E3. doi: 10.3171/2009.3.FOCUS0958. Neurosurg Focus. 2009. PMID: 19485716 Review.
Cited by
-
Is Spreading Depolarization a Risk Factor for Late Epilepsy? A Prospective Study in Patients with Traumatic Brain Injury and Malignant Ischemic Stroke Undergoing Decompressive Craniectomy.Neurocrit Care. 2021 Jun;34(3):876-888. doi: 10.1007/s12028-020-01107-x. Epub 2020 Sep 30. Neurocrit Care. 2021. PMID: 33000378
-
Craniectomy Combined with Rapid Internal Decompression in Massive Cerebral Infarction : Surgical Technique and Outcomes.J Korean Neurosurg Soc. 2025 Jul;68(4):405-414. doi: 10.3340/jkns.2024.0210. Epub 2025 May 23. J Korean Neurosurg Soc. 2025. PMID: 40404343 Free PMC article.
-
Hospital Revisits for Post-Ischemic Stroke Epilepsy after Acute Stroke Interventions.J Stroke Cerebrovasc Dis. 2022 Jan;31(1):106155. doi: 10.1016/j.jstrokecerebrovasdis.2021.106155. Epub 2021 Oct 21. J Stroke Cerebrovasc Dis. 2022. PMID: 34688213 Free PMC article.
-
Timing of Decompressive Craniectomy for Malignant Middle Cerebral Artery Infarction: A Single-Center Analysis.Medicina (Kaunas). 2019 Jan 30;55(2):31. doi: 10.3390/medicina55020031. Medicina (Kaunas). 2019. PMID: 30704138 Free PMC article.
-
Complications of Decompressive Craniectomy.Front Neurol. 2018 Nov 20;9:977. doi: 10.3389/fneur.2018.00977. eCollection 2018. Front Neurol. 2018. PMID: 30524359 Free PMC article. Review.
References
-
- Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet. 2008;371:1612–1623. - PubMed
-
- So EL, Annegers JF, Hauser WA, O'Brien PC, Whisnant JP. Population-based study of seizure disorders after cerebral infarction. Neurology. 1996;46:350–355. - PubMed
-
- Bladin CF, Alexandrov AV, Bellavance A, Bornstein N, Chambers B, Cote R, Lebrun L, Pirisi A, Norris JW. Seizures after stroke: a prospective multicenter study. Arch Neurol. 2000;57:1617–1622. - PubMed
-
- Lamy C, Domigo V, Semah F, Arquizan C, Trystram D, Coste J, Mas JL, Patent Foramen Ovale and Atrial Septal Aneurysm Study Group Early and late seizures after cryptogenic ischemic stroke in young adults. Neurology. 2003;60:400–404. - PubMed
-
- Krishnamurthi RV, Moran AE, Feigin VL, Barker-Collo S, Norrving B, Mensah GA, Taylor S, Naghavi M, Forouzanfar MH, Nguyen G, Johnson CO, Vos T, Murray CJ, Roth GA, GBD 2013 Stroke Panel Experts Group Stroke prevalence, mortality and disability-adjusted life years in adults aged 20–64 years in 1990–2013: data from the Global Burden of Disease 2013 Study. Neuroepidemiology. 2015;45:190–202. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
