

Evaluating wait times from screening to breast cancer diagnosis among women undergoing organised assessment vs usual care
- PMID: 28359079
- PMCID: PMC5482732
- DOI: 10.1038/bjc.2017.87
Evaluating wait times from screening to breast cancer diagnosis among women undergoing organised assessment vs usual care
Abstract
Background: Timely coordinated diagnostic assessment following an abnormal screening mammogram reduces patient anxiety and may optimise breast cancer prognosis. Since 1998, the Ontario Breast Screening Program (OBSP) has offered organised assessment through Breast Assessment Centres (BACs). For OBSP women seen at a BAC, an abnormal mammogram is followed by coordinated referrals through the use of navigators for further imaging, biopsy, and surgical consultation as indicated. For OBSP women seen through usual care (UC), further diagnostic imaging is arranged directly from the screening centre and/or through their physician; results must be communicated to the physician who is then responsible for arranging any necessary biopsy and/or surgical consultation. This study aims to evaluate factors associated with diagnostic wait times for women undergoing assessment through BAC and UC.
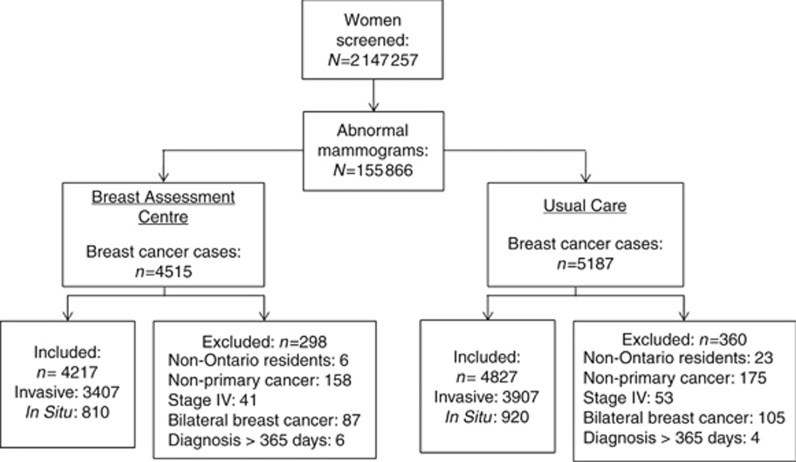
Methods: Of the 2 147 257 women aged 50-69 years screened in the OBSP between 1 January 2002 and 31 December 2009, 155 866 (7.3%) had an abnormal mammogram. A retrospective design identified two concurrent cohorts of women diagnosed with screen-detected breast cancer at a BAC (n=4217; 47%) and UC (n=4827; 53%). Multivariable logistic regression analyses examined associations between wait times and assessment and prognostic characteristics by pathway. A two-sided 5% significance level was used.
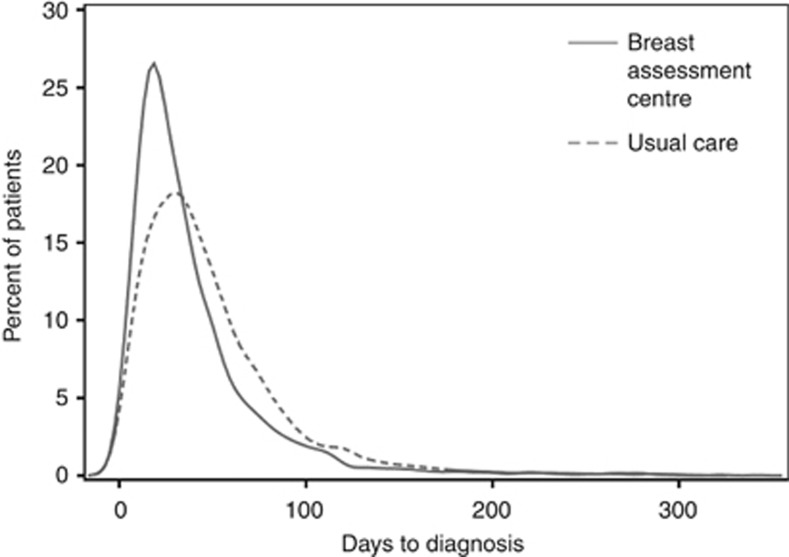
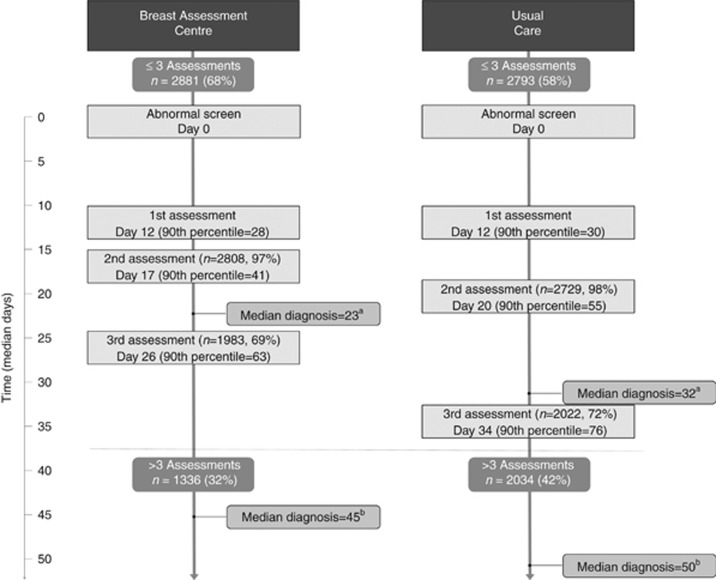
Results: Screened women with breast cancer were two times more likely to be diagnosed within 7 weeks when assessed through a BAC vs UC (OR=1.91, 95% CI=1.73-2.10). In addition, compared with UC, women assessed through a BAC were significantly more likely to have their first assessment procedure within 3 weeks of their abnormal mammogram (OR=1.25, 95% CI=1.12-1.39), ⩽3 assessment procedures (OR=1.54, 95% CI=1.41-1.69), ⩽2 assessment visits (OR=1.86, 95% CI=1.70-2.05), and ⩾2 procedures per visit (OR=1.41, 95% CI=1.28-1.55). Women diagnosed through a BAC were also more likely than those in UC to have imaging (OR=1.99, 95% CI=1.44-2.75) or a biopsy (OR=3.69, 95% CI=2.64-5.15) vs consultation only at their first assessment visit, and two times more likely to have a core or FNA biopsy than a surgical biopsy (OR=2.08, 95% CI=1.81-2.40). Having ⩽2 assessment visits was more likely to reduce time to diagnosis for women assessed through a BAC compared with UC (BAC OR=10.58, 95% CI=8.96-12.50; UC OR=4.47, 95% CI=3.94-5.07), as was having ⩽3 assessment procedures (BAC OR=4.97, 95% CI=4.26-5.79; UC OR=2.95, 95% CI=2.61-3.33). Income quintile affected wait times only in women diagnosed in UC, with those in the two highest quintiles more likely to receive a diagnosis in 7 weeks.
Conclusions: Women with screen-detected breast cancer in OBSP were more likely to have shorter wait times if they were diagnosed through organised assessment. This might be as a result of women diagnosed through a BAC having more procedures per visit, procedures scheduled in shorter intervals, and imaging or biopsy on their first visit. Given the significant improvement in timeliness to diagnosis, women with abnormal mammograms should be managed through organised assessment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Allen JD, Shelton RC, Harden E, Goldman RE (2008) Follow-up of abnormal screening mammograms among low-income ethnically diverse women: findings from a qualitative study. Patient Educ Couns 72: 283–292. - PubMed
-
- American Joint Committee on Cancer (2002) Cancer Staging Manual 6th edn Springer-Verlag: New York.
-
- Bairati I, Jobin E, Fillion L, Larochelle M, Vincent L (2007) Determinants of delay for breast cancer diagnosis. Cancer Detect Prev 31: 323–331. - PubMed
-
- Baliski C, Mcgahan CE, Liberto CM, Broughton S, Ellard S, Taylor M, Bates J, Lai A (2014) Influence of nurse navigation on wait times for breast cancer care in a Canadian regional cancer center. Am J Surg 207: 686–692. - PubMed
-
- Bevers TB, Anderson BO, Bonaccio E, Buys S, Daly MB, Dempsey PJ, Farrar WB, Fleming I, Garber JE, Harris RE, Heerdt AS, Helvie M, Huff JG, Khakpour N, Khan SA, Krontiras H, Lyman G, Rafferty E, Shaw S, Smith ML, Tsangaris TN, Williams C, Yankeelov T National Comprehensive Cancer Network (2009) NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw 7: 1060–1096. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
