

A Perspective on Middle-Aged and Older Men With Functional Hypogonadism: Focus on Holistic Management
- PMID: 28359097
- PMCID: PMC5477803
- DOI: 10.1210/jc.2016-3580
A Perspective on Middle-Aged and Older Men With Functional Hypogonadism: Focus on Holistic Management
Abstract
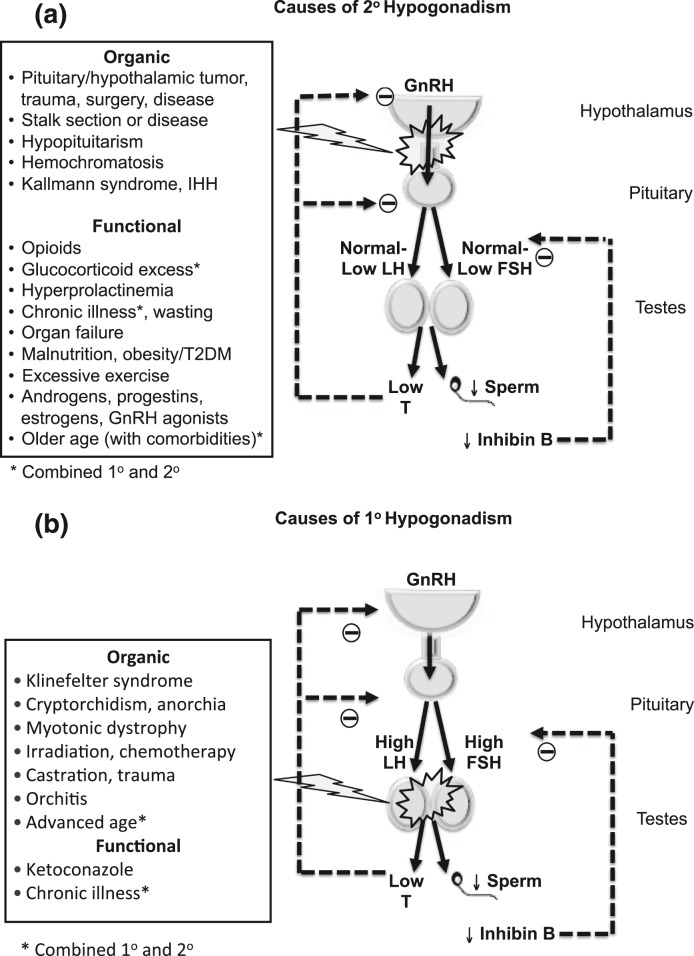
Context: Middle-aged and older men (≥50 years), especially those who are obese and suffer from comorbidities, not uncommonly present with clinical features consistent with androgen deficiency and modestly reduced testosterone levels. Commonly, such men do not demonstrate anatomical hypothalamic-pituitary-testicular axis pathology but have functional hypogonadism that is potentially reversible.
Evidence acquisition: Literature review from 1970 to October 2016.
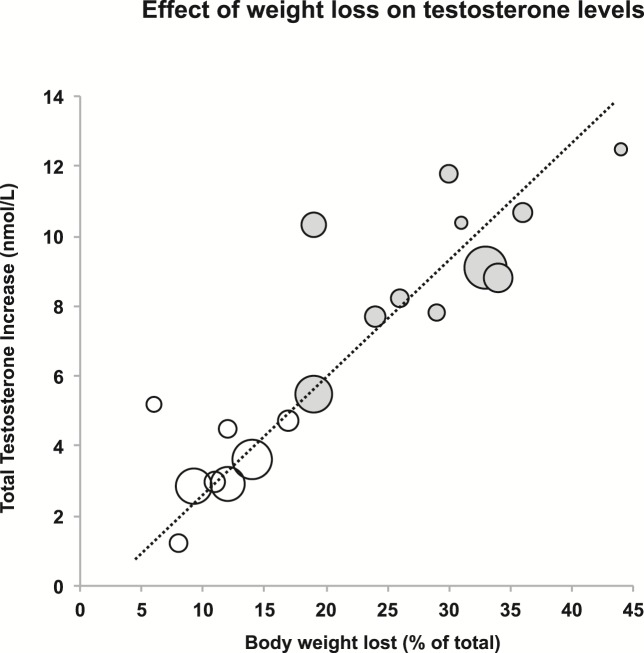
Evidence synthesis: Although definitive randomized controlled trials are lacking, evidence suggests that in such men, lifestyle measures to achieve weight loss and optimization of comorbidities, including discontinuation of offending medications, lead to clinical improvement and a modest increase in testosterone. Also, androgen deficiency-like symptoms and end-organ deficits respond to targeted treatments (such as phosphodiesterase-5 inhibitors for erectile dysfunction) without evidence that hypogonadal men are refractory. Unfortunately, lifestyle interventions remain difficult and may be insufficient even if successful. Testosterone therapy should be considered primarily for men who have significant clinical features of androgen deficiency and unequivocally low testosterone levels. Testosterone should be initiated either concomitantly with a trial of lifestyle measures, or after such a trial fails, after a tailored diagnostic work-up, exclusion of contraindications, and appropriate counseling.
Conclusions: There is modest evidence that functional hypogonadism responds to lifestyle measures and optimization of comorbidities. If achievable, these interventions may have demonstrable health benefits beyond the potential for increasing testosterone levels. Therefore, treatment of underlying causes of functional hypogonadism and of symptoms should be used either as an initial or adjunctive approach to testosterone therapy.
Figures
References
-
- Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM; Task Force, Endocrine Society . Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536–2559. - PubMed
-
- Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morales A, Morley JE, Schulman C, Thompson IM, Weidner W, Wu FC; International Society of Andrology (ISA); International Society for the Study of Aging Male (ISSAM); European Association of Urology (EAU); European Academy of Andrology (EAA); American Society of Andrology (ASA) . Investigation, treatment, and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA, and ASA recommendations. J Androl. 2009;30(1):1–9. - PubMed
-
- Bojesen A, Juul S, Gravholt CH. Prenatal and postnatal prevalence of Klinefelter syndrome: a national registry study. J Clin Endocrinol Metab. 2003;88(2):622–626. - PubMed
-
- Harman SM, Tsitouras PD. Reproductive hormones in aging men. I. Measurement of sex steroids, basal luteinizing hormone, and Leydig cell response to human chorionic gonadotropin. J Clin Endocrinol Metab. 1980;51(1):35–40. - PubMed
-
- Neaves WB, Johnson L, Porter JC, Parker CR Jr, Petty CS. Leydig cell numbers, daily sperm production, and serum gonadotropin levels in aging men. J Clin Endocrinol Metab. 1984;59(4):756–763. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
