

Effects of chalazia on corneal astigmatism : Large-sized chalazia in middle upper eyelids compress the cornea and induce the corneal astigmatism
- PMID: 28359272
- PMCID: PMC5374600
- DOI: 10.1186/s12886-017-0426-2
Effects of chalazia on corneal astigmatism : Large-sized chalazia in middle upper eyelids compress the cornea and induce the corneal astigmatism
Abstract
Background: A chalazion is a common eyelid disease that causes eye morbidity due to inflammation and cosmetic disfigurement. Corneal topographic changes are important factors in corneal refractive surgery, intraocular lens power calculations for cataract surgery, and visual acuity assessments. However, the effects of chalazia on corneal astigmatism have not been thoroughly investigated. The changes in corneal astigmatism according to chalazion size and location is necessary for better outcome of ocular surgery. The aim of this study is to evaluate changes in corneal astigmatism according to chalazion size and location.
Methods: In this cross-sectional study, a total of 44 eyes from 33 patients were included in the chalazion group and 70 eyes from 46 patients comprised the control group. Chalazia were classified according to location and size. An autokeratorefractometer (KR8100, Topcon; Japan) and a Galilei™ dual-Scheimpflug analyzer (Ziemer Group; Port, Switzerland) were utilized to evaluate corneal changes.
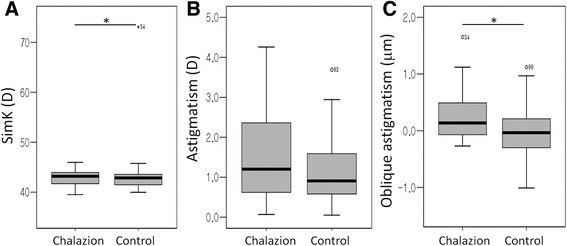
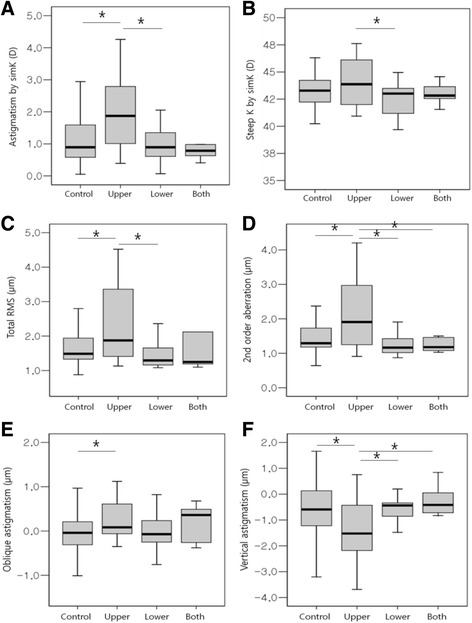
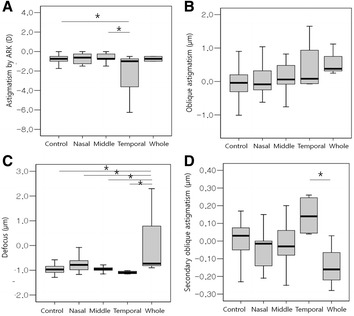
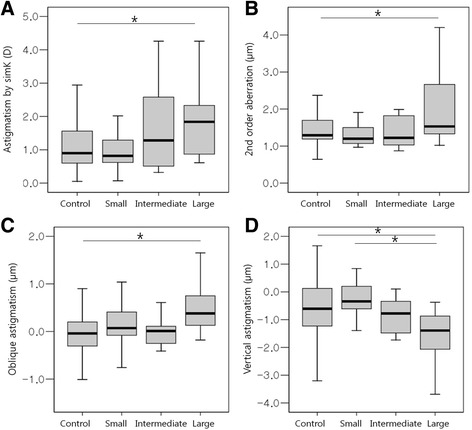
Result: Oblique astigmatism was greater in the chalazion group compared with the control group (p < 0.05). Astigmatism by simulated keratometry (simK), steep K by simK, total root mean square, second order aberration, oblique astigmatism, and vertical astigmatism were significantly greater in the upper eyelid group (p < 0.05). Astigmatism by simK, second order aberration, oblique astigmatism, and vertical astigmatism were significantly greater in the large-sized chalazion group (p < 0.05). Corneal wavefront aberration was the greatest in the upper eyelid chalazion group, whole area group, and large-sized chalazion group (p < 0.05).
Conclusions: Large-sized chalazia in the whole upper eyelid should be treated in the early phase because they induced the greatest change in corneal topography. Chalazion should be treated before corneal topography is performed preoperatively and before the diagnosis of corneal diseases.
Keywords: Astigmatism; Chalazia; Corneal topography; Wavefront.
Figures
References
-
- Goawalla A, Lee V. A prospective randomized treatment study comparing three treatment options for chalazia: triamcinolone acetonide injections, incision and curettage and treatment with hot compresses. Clin Experiment Ophthalmol. 2007;35:706–712. doi: 10.1111/j.1442-9071.2007.01617.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
