

Leg pain location and neurological signs relate to outcomes in primary care patients with low back pain
- PMID: 28359275
- PMCID: PMC5374567
- DOI: 10.1186/s12891-017-1495-3
Leg pain location and neurological signs relate to outcomes in primary care patients with low back pain
Abstract
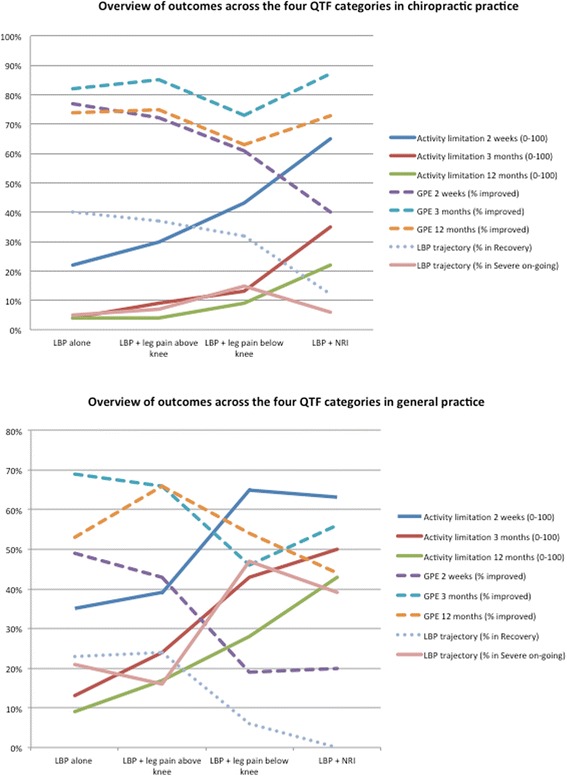
Background: Low back pain (LBP) patients with related leg pain and signs of nerve root involvement are considered to have a worse prognosis than patients with LBP alone. However, it is unclear whether leg pain location above or below the knee and the presence of neurological signs are important in primary care patients. The objectives of this study were to explore whether the four Quebec Task Force categories (QTFC) based on the location of pain and on neurological signs have different characteristics at the time of care seeking, whether these QTFC are associated with outcome, and if so whether there is an obvious ranking of the four QTFC on the severity of outcomes.
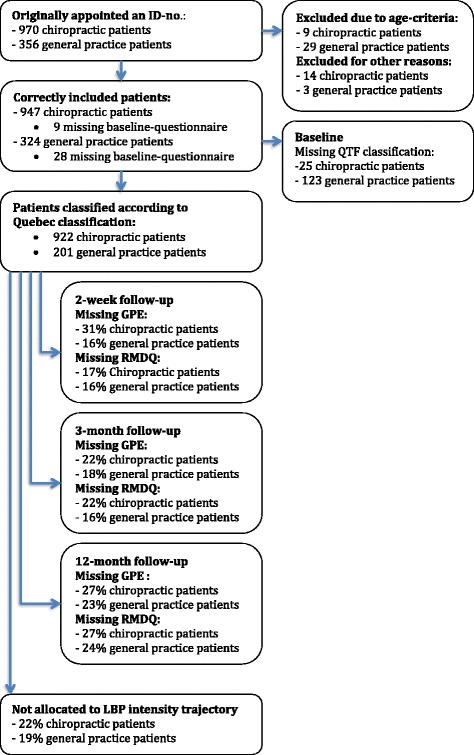
Method: Adult patients seeking care for LBP in chiropractic or general practice were classified into the four QTFC based on self-reported information and clinical findings. Analyses were performed to test the associations between the QTFC and baseline characteristics as well as the outcomes global perceived effect and activity limitation after 2 weeks, 3 months, and 1 year and also 1-year trajectories of LBP intensity.
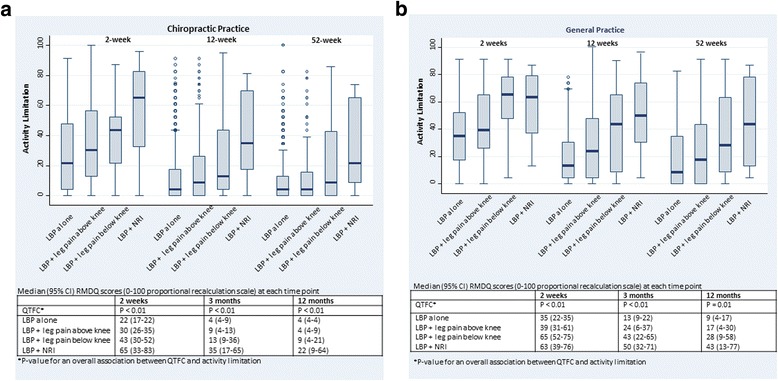
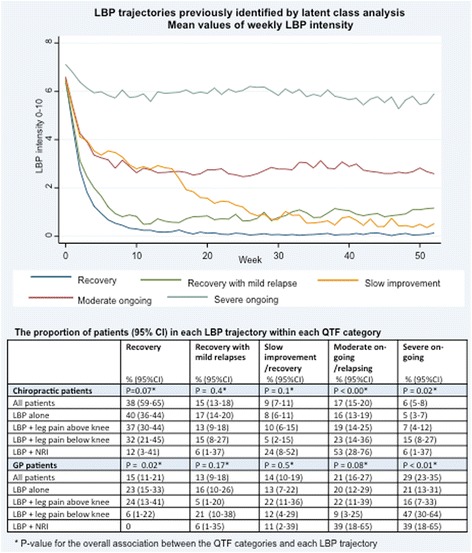
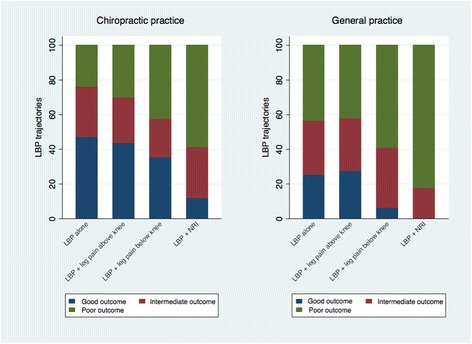
Results: The study comprised 1271 patients; 947 from chiropractic practice and 324 from general practice. The QTFC at presentation were statistically significantly associated with most of the baseline characteristics, with activity limitation at all follow-up time points, with global perceived effect at 2 weeks but not 3 months and 1 year, and with trajectories of LBP. Severity of outcomes in the QTFC increased from LBP alone, across LBP with leg pain above the knee and below the knee to LBP with nerve root involvement. However, the variation within the categories was considerable.
Conclusion: The QTFC identify different LBP subgroups at baseline and there is a consistent ranking of the four categories with respect to outcomes. The differences between outcomes appear to be large enough for the QTFC to be useful for clinicians in the communication with patients. However, due to variation of outcomes within each category individuals' outcome cannot be precisely predicted from the QTFC alone. It warrants further investigation to find out if the QTFC can improve existing prediction tools and guide treatment decisions.
Keywords: Classification; Cohort studies; Low back pain; Primary care; Quebec Task Force classification; Radiculopathy; Referred leg pain; Sciatica.
Figures
Similar articles
-
Prognostic implications of the Quebec Task Force classification of back-related leg pain: an analysis of longitudinal routine clinical data.BMC Musculoskelet Disord. 2013 May 24;14:171. doi: 10.1186/1471-2474-14-171. BMC Musculoskelet Disord. 2013. PMID: 23705775 Free PMC article.
-
Patients with low back pain differ from those who also have leg pain or signs of nerve root involvement - a cross-sectional study.BMC Musculoskelet Disord. 2012 Nov 28;13:236. doi: 10.1186/1471-2474-13-236. BMC Musculoskelet Disord. 2012. PMID: 23190800 Free PMC article.
-
Clinical outcomes among low back pain consulters with referred leg pain in primary care.Spine (Phila Pa 1976). 2011 Dec 1;36(25):2168-75. doi: 10.1097/BRS.0b013e31820712bb. Spine (Phila Pa 1976). 2011. PMID: 21358478
-
Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis.J Manipulative Physiol Ther. 2008 Nov-Dec;31(9):659-74. doi: 10.1016/j.jmpt.2008.10.007. J Manipulative Physiol Ther. 2008. PMID: 19028250 Review.
-
Guidelines for clinical studies assessing the efficacy of drugs for the management of acute low back pain.Clin Exp Rheumatol. 2003 Nov-Dec;21(6):691-4. Clin Exp Rheumatol. 2003. PMID: 14740445 Review.
Cited by
-
Physical Therapy Referral From Primary Care for Acute Back Pain With Sciatica : A Randomized Controlled Trial.Ann Intern Med. 2021 Jan;174(1):8-17. doi: 10.7326/M20-4187. Epub 2020 Oct 6. Ann Intern Med. 2021. PMID: 33017565 Free PMC article. Clinical Trial.
-
Initial pain and disability characteristics can assist the prediction of the centralization phenomenon on initial assessment of patients with low back pain.J Man Manip Ther. 2019 May;27(2):66-72. doi: 10.1080/10669817.2018.1542560. Epub 2018 Nov 5. J Man Manip Ther. 2019. PMID: 30935340 Free PMC article.
-
The Danish Chiropractic Low Back Pain Cohort (ChiCo): Description and Summary of an Available Data Source for Research Collaborations.Clin Epidemiol. 2020 Oct 2;12:1015-1027. doi: 10.2147/CLEP.S266220. eCollection 2020. Clin Epidemiol. 2020. PMID: 33061649 Free PMC article.
-
Guideline adherence and socioeconomic factors in Danish patients referred to secondary care for low back pain: a cross sectional study.BMC Public Health. 2023 Sep 6;23(1):1733. doi: 10.1186/s12889-023-16633-4. BMC Public Health. 2023. PMID: 37674149 Free PMC article.
-
Patient expectations and levels of satisfaction in chiropractic treatment for lumbar radiculopathy. A mixed methods study.Chiropr Man Therap. 2023 May 19;31(1):13. doi: 10.1186/s12998-023-00486-0. Chiropr Man Therap. 2023. PMID: 37208689 Free PMC article.
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- United States Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States (BMUS) TE, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed 3 May 2016.
-
- Flachs EM EL, Koch MB, Ryd JT, Dibba E, Skov-Ettrup L, Juel K. Statens Institut for Folkesundhed, Syddansk Universitet. København: Sundhedsstyrelsen; 2015. Sygdomsbyrden i Danmark – sygdomme.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
