

First Application of 7-T Magnetic Resonance Imaging in Endoscopic Endonasal Surgery of Skull Base Tumors
- PMID: 28359922
- PMCID: PMC5819330
- DOI: 10.1016/j.wneu.2017.03.088
First Application of 7-T Magnetic Resonance Imaging in Endoscopic Endonasal Surgery of Skull Base Tumors
Abstract
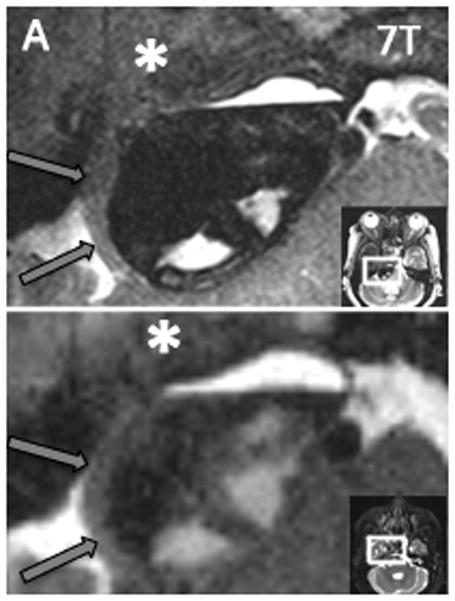
Background: Successful endoscopic endonasal surgery for the resection of skull base tumors is reliant on preoperative imaging to delineate pathology from the surrounding anatomy. The increased signal-to-noise ratio afforded by 7-T MRI can be used to increase spatial and contrast resolution, which may lend itself to improved imaging of the skull base. In this study, we apply a 7-T imaging protocol to patients with skull base tumors and compare the images with clinical standard of care.
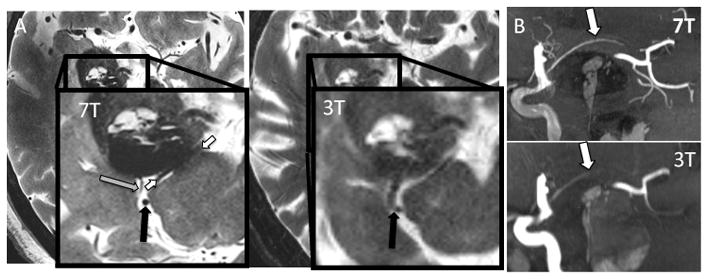
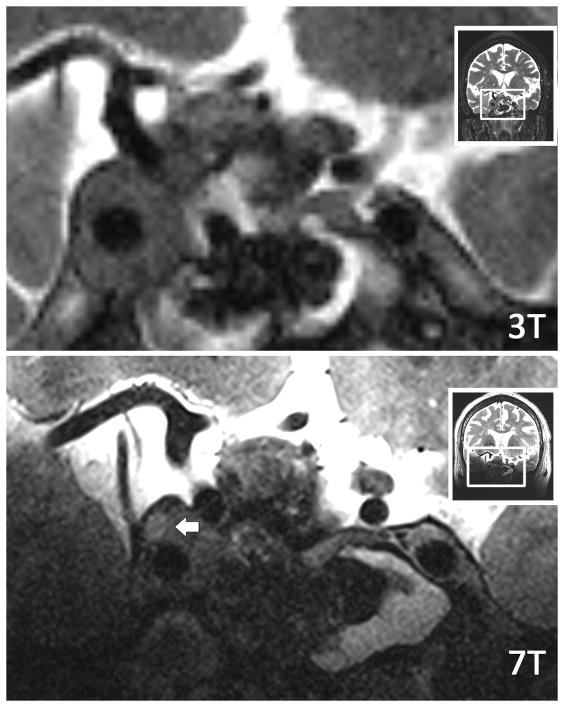
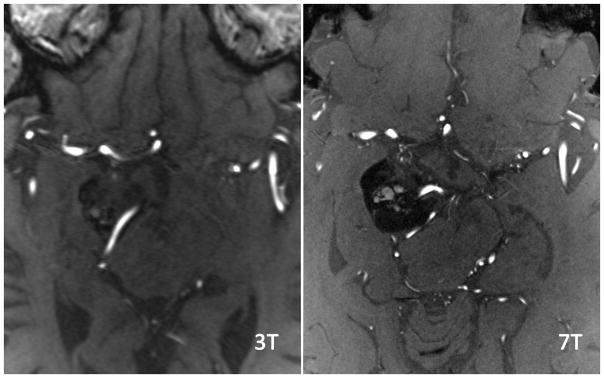
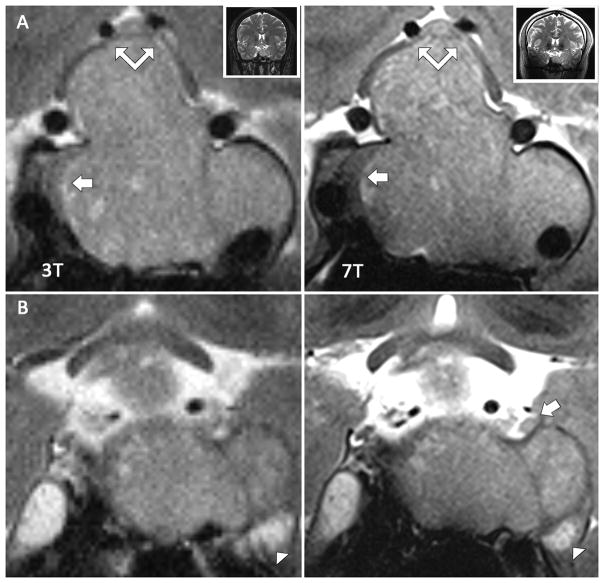
Methods: Images were acquired at 7 T on 11 patients with skull base lesions. Two neuroradiologists evaluated clinical 1.5-, 3-, and 7-T scans for detection of intracavernous cranial nerves and internal carotid artery (ICA) branches. Detection rates were compared. Images were used for surgical planning and uploaded to a neuronavigation platform and used to guide surgery.
Results: Image analysis yielded improved detection rates of cranial nerves and ICA branches at 7 T. The 7-T images were successfully incorporated into preoperative planning and intraoperative neuronavigation.
Conclusions: Our study represents the first application of 7-T MRI to the full neurosurgical workflow for endoscopic endonasal surgery. We detected higher rates of cranial nerves and ICA branches at 7-T MRI compared with 3- and 1.5-T MRI, and found that integration of 7 T into surgical planning and guidance was feasible. These results suggest a potential for 7-T MRI to reduce surgical complications. Future studies comparing standardized 7-, 3-, and 1.5-T MRI protocols in a larger number of patients are warranted to determine the relative benefit of 7-T MRI for endonasal endoscopic surgical efficacy.
Keywords: 7-T MRI; Endoscopic endonasal surgery; Skull base tumors; Ultrahigh-field MRI.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures

References
-
- Alimohamadi M, Sanjari R, Mortazavi A, Shirani M, Moradi Tabriz H, Hadizadeh Kharazi H, et al. Predictive value of diffusion-weighted MRI for tumor consistency and resection rate of nonfunctional pituitary macroadenomas. Acta Neurochir (Wien) 2014;156:2245–2252. discussion 2252. - PubMed
-
- Amemiya S, Aoki S, Ohtomo K. Cranial nerve assessment in cavernous sinus tumors with contrast-enhanced 3D fast-imaging employing steady-state acquisition MR imaging. Neuroradiology. 2009;51:467–470. - PubMed
-
- Barrett TF, Sarkiss CA, Dyvorne HA, Lee J, Balchandani P, Shrivastava RK. Application of Ultrahigh Field Magnetic Resonance Imaging in the Treatment of Brain Tumors: A Meta-Analysis. World Neurosurg. 2016;86:450–465. - PubMed
-
- Blitz AM, Aygun N, Herzka DA, Ishii M, Gallia GL. High Resolution Three-Dimensional MR Imaging of the Skull Base: Compartments, Boundaries, and Critical Structures. Radiol Clin North Am. 2017;55:17–30. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
