

Biomarker Profiles in Heart Failure Patients With Preserved and Reduced Ejection Fraction
- PMID: 28360225
- PMCID: PMC5532986
- DOI: 10.1161/JAHA.116.003989
Biomarker Profiles in Heart Failure Patients With Preserved and Reduced Ejection Fraction
Abstract
Background: Biomarkers may help us to unravel differences in the underlying pathophysiology between heart failure (HF) patients with a reduced ejection fraction (HFrEF) and a preserved ejection fraction (HFpEF). Therefore, we compared biomarker profiles to characterize pathophysiological differences between patients with HFrEF and HFpEF.
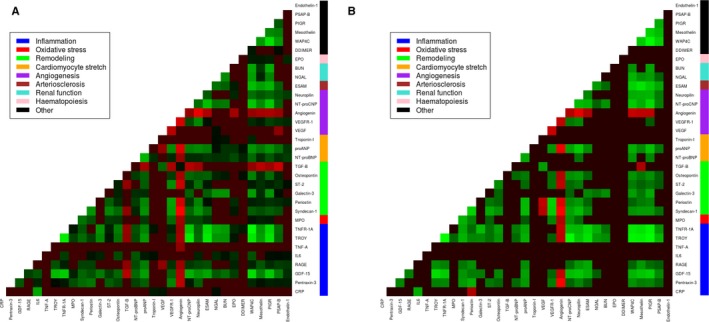
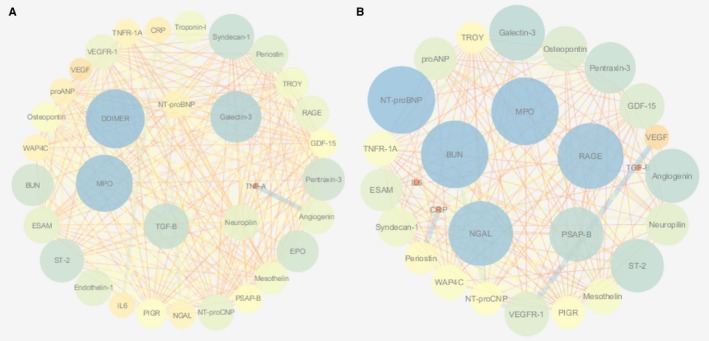
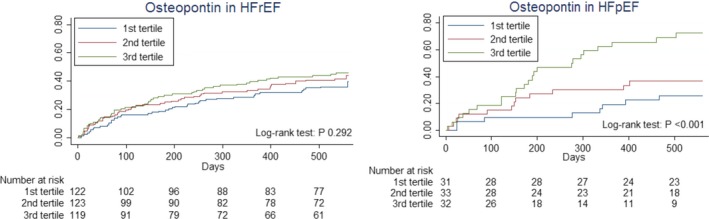
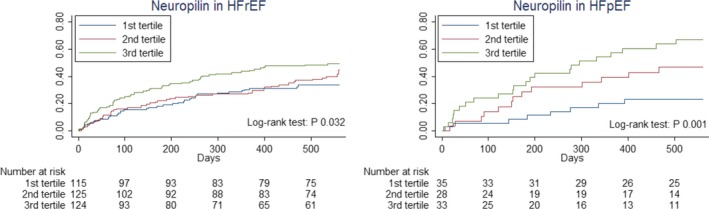
Methods and results: We retrospectively analyzed 33 biomarkers from different pathophysiological domains (inflammation, oxidative stress, remodeling, cardiac stretch, angiogenesis, arteriosclerosis, and renal function) in 460 HF patients (21% HFpEF, left ventricular ejection fraction ≥45%) measured at discharge after hospitalization for acute HF. The association between these markers and the occurrence of all-cause mortality and/or HF-related rehospitalizations at 18 months was compared between patients with HFrEF and HFpEF. Patients were 70.6±11.4 years old and 37.4% were female. Patients with HFpEF were older, more often female, and had a higher systolic blood pressure. Levels of high-sensitive C-reactive protein were significantly higher in HFpEF, while levels of pro-atrial-type natriuretic peptide and N-terminal pro-brain natriuretic peptide were higher in HFrEF. Linear regression followed by network analyses revealed prominent inflammation and angiogenesis-associated interactions in HFpEF and mainly cardiac stretch-associated interactions in HFrEF. The angiogenesis-specific marker, neuropilin and the remodeling-specific marker, osteopontin were predictive for all-cause mortality and/or HF-related rehospitalizations at 18 months in HFpEF, but not in HFrEF (P for interaction <0.05).
Conclusions: In HFpEF, inflammation and angiogenesis-mediated interactions are predominantly observed, while stretch-mediated interactions are found in HFrEF. The remodeling marker osteopontin and the angiogenesis marker neuropilin predicted outcome in HFpEF, but not in HFrEF.
Keywords: biomarker; heart failure; multimarker; pathophysiology.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- van Veldhuisen DJ, Cohen‐Solal A, Böhm M, Anker SD, Babalis D, Roughton M, Coats AJS, Poole‐Wilson PA, Flather MD. Beta‐blockade with nebivolol in elderly heart failure patients with impaired and preserved left ventricular ejection fraction: data from SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure). J Am Coll Cardiol. 2009;53:2150–2158. - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, Olofsson B, Ostergren J; Committees CI . Effects of candesartan in patients with chronic heart failure and preserved left‐ventricular ejection fraction: the CHARM‐Preserved Trial. Lancet. 2003;362:777–781. - PubMed
-
- Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, Clausell N, Desai AS, Diaz R, Fleg JL, Gordeev I, Harty B, Heitner JF, Kenwood CT, Lewis EF, O'Meara E, Probstfield JL, Shaburishvili T, Shah SJ, Solomon SD, Sweitzer NK, Yang S, McKinlay SM; Investigators T . Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370:1383–1392. - PubMed
-
- Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148–2159. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
