

Aortic Calcification Onset and Progression: Association With the Development of Coronary Atherosclerosis
- PMID: 28360229
- PMCID: PMC5533012
- DOI: 10.1161/JAHA.116.005093
Aortic Calcification Onset and Progression: Association With the Development of Coronary Atherosclerosis
Abstract
Background: Thoracic aortic calcification (TAC) and coronary artery calcification (CAC) are markers of subclinical atherosclerosis and are associated with incident major cardiovascular events. We investigated major determinants for incidence and progression of TAC and the association between TAC and CAC incidence and progression.
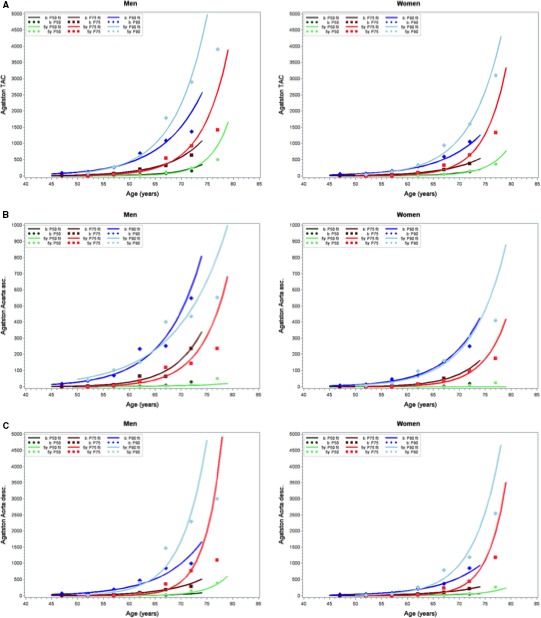
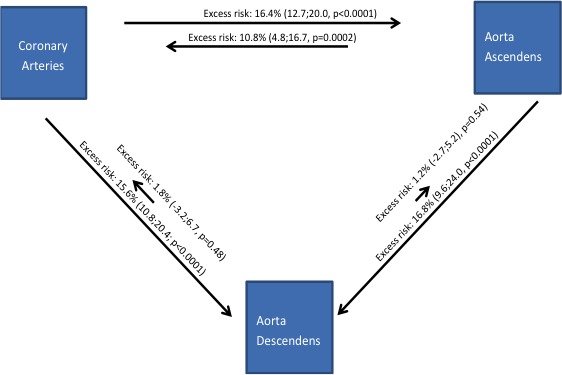
Methods and results: In a population-based cohort study, 3270 participants (aged 45-74 years, 53.1% women) received cardiac computed tomography at baseline and after a mean follow-up of 5.1±0.3 years for quantification of calcification of the ascending (ATAC) and descending thoracic aorta (DTAC) and CAC. Multivariable relative risk regression analysis was used to investigate associations of cardiovascular risk factors with incident TAC, of baseline TAC with incident CAC, and of baseline CAC with incident TAC. Of 1243 participants with baseline TAC of 0, 517 (41.6%) revealed incident TAC after 5 years. Incidence of descending TAC was higher (34.5%) than ascending TAC (23.3%). Incident TAC after 5 years was associated with age (relative risk 1.26 [95% CI 1.21-1.33], per 5 years), blood pressure (relative risk 1.06 [95% CI 1.03-1.10], per 10 mm Hg), low-density lipoprotein cholesterol (relative risk 1.08 [95% CI 1.04-1.12], per 20 mg/dL), and smoking (relative risk 1.28 [95% CI 1.07-1.53]). Among the 1185 participants without CAC at baseline, the risk of developing CAC was 28.3% when baseline TAC was present compared with 22.2% among those without baseline TAC (excess risk 6.1% [95% CI 1.2-11.0%]). The point estimate of excess risk for incident CAC was higher for ascending TAC (10.8% [95% CI 4.8-16.7%]) and low for descending TAC (1.8% [95% CI -3.2% to 6.7%]). Excess risk for developing ascending and descending TAC with present baseline CAC was 16.4% (95% CI 12.7-20.0%) and 15.6% (95% CI 10.8-20.4%), respectively.
Conclusion: TAC and CAC share similar major determinants for incident calcification. Participants with TAC, especially ascending TAC, are at elevated risk for development of CAC.
Keywords: aortic disease; calcification; cardiac CT; computed tomography; coronary artery calcification; thoracic aortic calcification.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Kälsch H, Lehmann N, Möhlenkamp S, Hammer C, Mahabadi AA, Moebus S, Schmermund A, Stang A, Bauer M, Jöckel KH, Erbel R; Investigator Group of the Heinz Nixdorf Recall Study . Prevalence of thoracic aortic calcification and its relationship to cardiovascular risk factors and coronary calcification in an unselected population‐based cohort—the Heinz Nixdorf Recall Study. Int J Cardiovasc Imaging. 2013;29:207–216. - PubMed
-
- Schmermund A, Möhlenkamp S, Stang A, Grönemeyer D, Seibel R, Hirche H, Mann K, Siffert W, Lauterbach K, Siegrist J, Jöckel KH, Erbel R; Heinz Nixdorf Recall Study Investigative Group . Assessment of clinically silent atherosclerotic disease and established and novel risk factors for predicting myocardial infarction and cardiac death in healthy middle‐aged subjects: rationale and design of the Heinz Nixdorf Recall Study. Am Heart J. 2002;144:212–218. - PubMed
-
- Kälsch H, Hennig F, Moebus S, Möhlenkamp S, Dragano N, Jakobs H, Memmesheimer M, Erbel R, Jöckel KH, Hoffmann B; Heinz Nixdorf Recall Study Investigative Group . Are air pollution and traffic noise independently associated with atherosclerosis: the Heinz Nixdorf Recall Study. Eur Heart J. 2014;35:853–860. - PubMed
-
- Erbel R, Möhlenkamp S, Moebus S, Schmermund A, Lehmann N, Stang A, Dragano N, Grönemeyer D, Seibel R, Kälsch H, Bröcker‐Preuss M, Mann K, Siegrist J, Jöckel KH; Heinz Nixdorf Recall Study Investigative Group . Coronary risk stratification, discrimination, and reclassification improvement based on quantification of subclinical coronary atherosclerosis: the Heinz Nixdorf Recall Study. J Am Coll Cardiol. 2010;56:1397–1406. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
