

Alternative remedies for insomnia: a proposed method for personalized therapeutic trials
- PMID: 28360539
- PMCID: PMC5364017
- DOI: 10.2147/NSS.S128095
Alternative remedies for insomnia: a proposed method for personalized therapeutic trials
Abstract
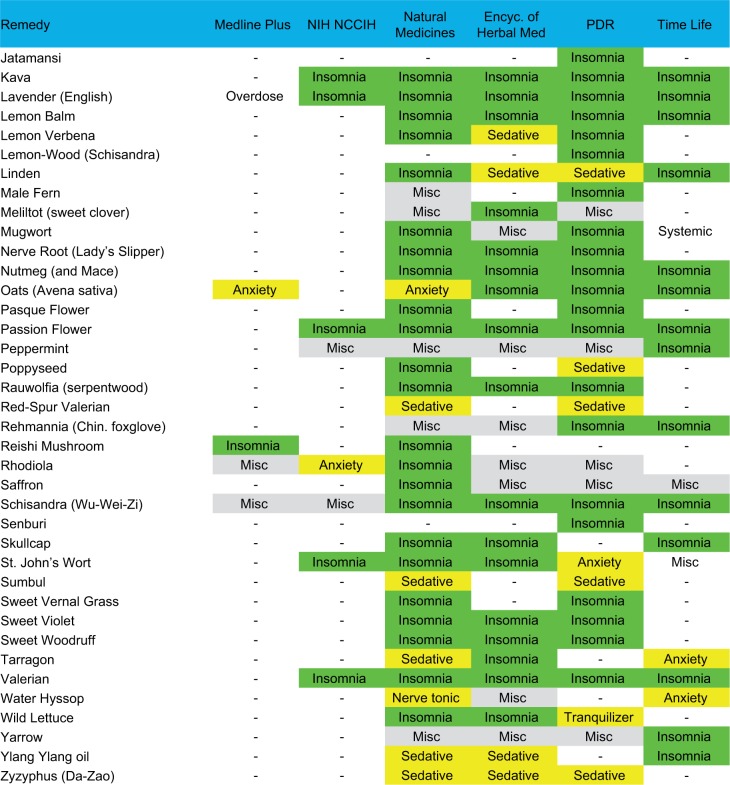
Insomnia is a common symptom, with chronic insomnia being diagnosed in 5-10% of adults. Although many insomnia patients use prescription therapy for insomnia, the health benefits remain uncertain and adverse risks remain a concern. While similar effectiveness and risk concerns exist for herbal remedies, many individuals turn to such alternatives to prescriptions for insomnia. Like prescription hypnotics, herbal remedies that have undergone clinical testing often show subjective sleep improvements that exceed objective measures, which may relate to interindividual heterogeneity and/or placebo effects. Response heterogeneity can undermine traditional randomized trial approaches, which in some fields has prompted a shift toward stratified trials based on genotype or phenotype, or the so-called n-of-1 method of testing placebo versus active drug in within-person alternating blocks. We reviewed six independent compendiums of herbal agents to assemble a group of over 70 reported to benefit sleep. To bridge the gap between the unfeasible expectation of formal evidence in this space and the reality of common self-medication by those with insomnia, we propose a method for guided self-testing that overcomes certain operational barriers related to inter- and intraindividual sources of phenotypic variability. Patient-chosen outcomes drive a general statistical model that allows personalized self-assessment that can augment the open-label nature of routine practice. The potential advantages of this method include flexibility to implement for other (nonherbal) insomnia interventions.
Keywords: alternative remedy; herbal; insomnia; over the counter; supplement.
Conflict of interest statement
Disclosure Dr Bianchi has received funding from the Department of Neurology, Massachusetts General Hospital, the Center for Integration of Medicine and Innovative Technology, the Milton Family Foundation, the MGH-MIT Grand Challenge, and the American Sleep Medicine Foundation. Dr Bianchi has a patent pending on a home sleep monitoring device. Dr Bianchi has research contracts with MC10 and Insomnisolv, a consulting agreement with McKesson and International Flavors and Fragrances, received payment for educational material from Oakstone Publishing, and has provided expert testimony in sleep medicine. Dr Bianchi serves as a medical monitor for Pfizer. Dr Westover has received funding from the NIH (NIH-NINDS 1K23NS090900). The other authors report no conflicts of interest in this work.
Figures




References
-
- Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6(2):97–111. - PubMed
-
- Espie CA, Luik AI, Cape J, et al. Digital cognitive behavioural therapy for insomnia versus sleep hygiene education: the impact of improved sleep on functional health, quality of life and psychological well-being. Study protocol for a randomised controlled trial. Trials. 2016;17(1):257. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
