

A Case of ADEM Mimicking Cerebral Adrenoleukodystrophy Based on Supratentorial MRI Findings
- PMID: 28360602
- PMCID: PMC5370266
- DOI: 10.4274/npa.y6886
A Case of ADEM Mimicking Cerebral Adrenoleukodystrophy Based on Supratentorial MRI Findings
Abstract
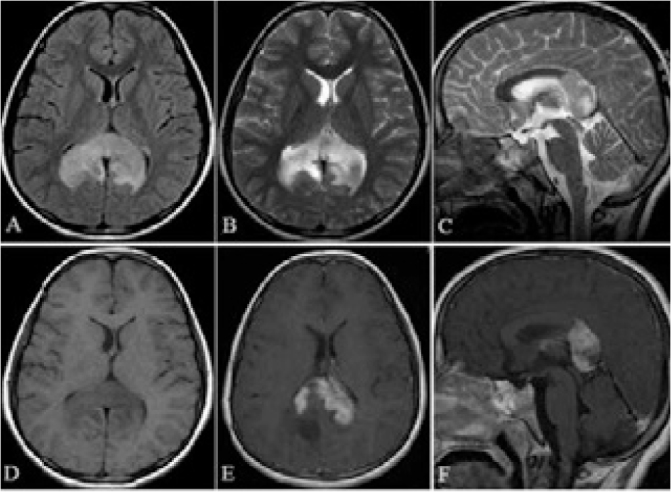
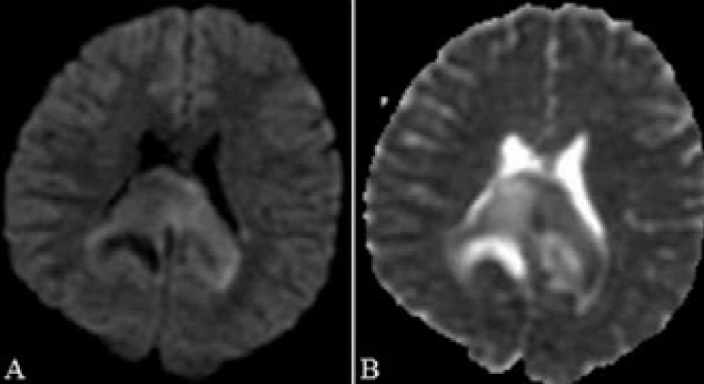
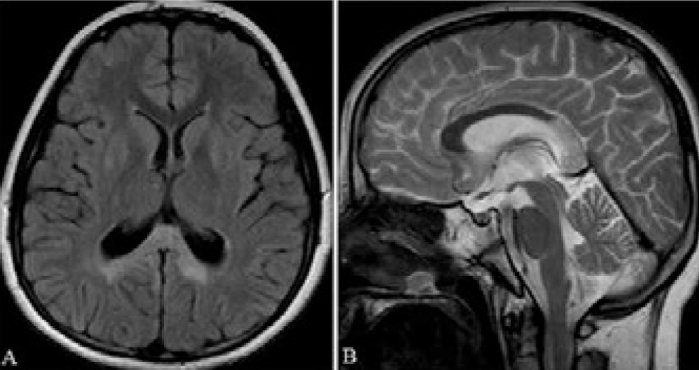
A 9-year-old male admitted for syncope also had the complains of pain and numbness in his legs and frequent falling down. There was a history of upper respiratory tract infection 10 days before. On neurologic examination, paraparesia and fall a sleep were identified. On magnetic resonance imaging, the symetric signal increases were seen in biparieto-occipital white matter intented to corpus callosum at T2-weighted sequences and cytotoxic edema was seen at diffusion-weighted images. Heterogeneous contrast enhancement was seen on these areas. In addition, at the C7-Th5 vertebrae levels, spinal cord had diffuse increased signal intensity and contrast enhancement. Acute disseminated encephalomyelitis was thought based on clinical and radiological findings. Steroid therapy was started. Significant improvement was shown after treatment. On 2-year follow-up, there was no recurrence. In conclusion, it must be kept in mind that acute disseminated encephalomyelitis can rarely present with biparieto-occipital involvement which extends to corpus callosum and can mimic adrenoleukodystrophy. For the differential diagnosis butterfly glioma, tumefactive demyelinating lesions or multiple sclerosis should be considered.
Bayılma nedeniyle getirilen dokuz yaşında erkek hastanın, ayrıca sık düşme, bacaklarında ağrı, uyuşukluk yakınması vardı. On gün öncesinde geçirilmiş üst solunum yolu enfeksiyonu öyküsü mevcuttu. Nörolojik muayenede, uykuya eğilim hali ve paraparezi saptandı. Manyetik rezonans görüntülemesinde T2 ağırlıklı kesitlerde korpus kallozumu içine alan biparieto-oksipital simetrik sinyal artışı ve difüzyon ağırlıklı incelemede sitotoksik ödem izlendi. Aynı alanlarda heterojen kontrast tutulumu dikkati çekmekteydi. Ayrıca omurilikte C7-T5 vertebra seviyelerinde kontrast tutulumu ve diffüz sinyal artışı mevcuttu. Hasta klinik ve radyolojik bulgular ile akut dissemine ensefalomiyelit olarak değerlendirildi. Steroid tedavisi başlandı. Tedavi sonrası belirgin düzelme izlendi. İki yıllık takibinde nüks görülmedi. Sonuç olarak akut dissemine ensefalomiyelitin nadirde olsa korpus kallozumu içine alan biparieto-oksipital tutulumla karşımıza çıkabileceği ve adrenolökodistrofi hastalığını taklit edebileceği akılda tutulmalıdır. Ayırıcı tanıda “butterfly” gliom, tümefaktif demiyelinizan lezyon veya multipl skleroz da unutulmamalıdır.
Keywords: Acute disseminated encephalomyelitis; Adrenoleukodystrophy; Leukodystrophy; MRI; Tumefactive demyelinating lesion.
Conflict of interest statement
Conflict of interest: The authors reported no conflict of interest related to this article. Çıkar Çatışması: Yazarlar bu makale ile ilgili olarak herhangi bir çıkar çatışması bildirmemişlerdir.
Figures

Similar articles
-
[Clinical features and neuroimaging findings of 12 patients with acute disseminated encephalomyelitis involved in corpus callosum].Zhonghua Yi Xue Za Zhi. 2012 Nov 20;92(43):3036-41. Zhonghua Yi Xue Za Zhi. 2012. PMID: 23328373 Chinese.
-
Evaluation of possible prognostic factors of fulminant acute disseminated encephalomyelitis (ADEM) on magnetic resonance imaging with fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging.Acta Radiol. 2009 Apr;50(3):334-9. doi: 10.1080/02841850902736617. Acta Radiol. 2009. PMID: 19235577
-
Callosal lesions on magnetic resonance imaging with multiple sclerosis, neuromyelitis optica spectrum disorder and acute disseminated encephalomyelitis.Mult Scler Relat Disord. 2019 Jul;32:41-45. doi: 10.1016/j.msard.2019.04.019. Epub 2019 Apr 16. Mult Scler Relat Disord. 2019. PMID: 31030018
-
Acute disseminated encephalomyelitis.J Child Neurol. 2012 Nov;27(11):1408-25. doi: 10.1177/0883073812455104. Epub 2012 Aug 21. J Child Neurol. 2012. PMID: 22914374 Review.
-
Acute disseminated encephalomyelitis.Postgrad Med J. 2003 Jan;79(927):11-7. doi: 10.1136/pmj.79.927.11. Postgrad Med J. 2003. PMID: 12566545 Free PMC article. Review.
References
-
- Lim KE, Hsu YY, Hsu WC, Chan CY. Multiple complete ring-shaped enhanced MRI lesions in acute disseminated encephalomyelitis. Clin Imaging. 2003;27:281–284. - PubMed
-
- Kawashima S, Matsukawa N, Ueki Y, Yamada K, Sakurai K, Yamawaki T, Ojika K. Predicting the motor outcome of acute disseminated encephalomyelitis by apparent diffusion coefficient imaging: Two case reports. J Neurol Sci. 2009;280:123–126. - PubMed
-
- Murthy SN, Faden HS, Cohen ME, Bakshi R. Acute disseminated encephalomyelitis in children. Pediatrics. 2002;110:e21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous