

Prevention and management of post-instability glenohumeral arthropathy
- PMID: 28361016
- PMCID: PMC5359759
- DOI: 10.5312/wjo.v8.i3.229
Prevention and management of post-instability glenohumeral arthropathy
Abstract
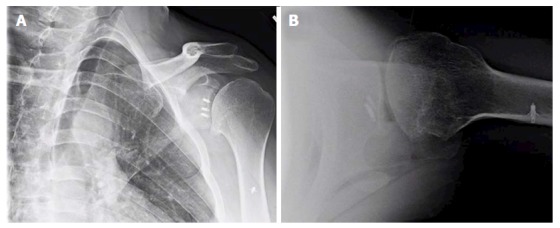
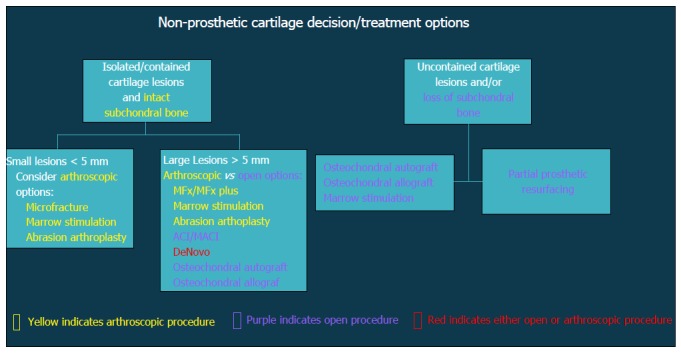
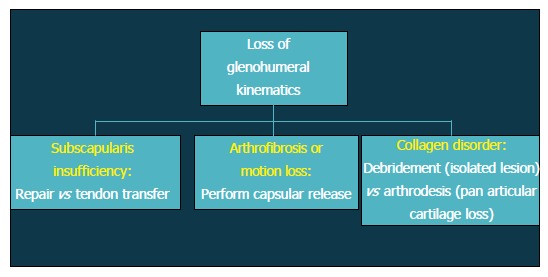
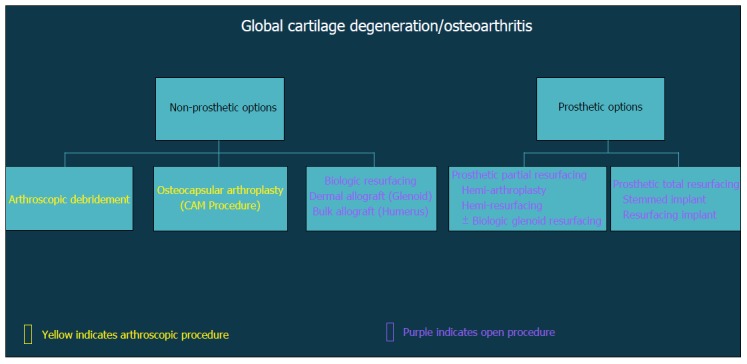
Post-instability arthropathy may commonly develop in high-risk patients with a history of recurrent glenohumeral instability, both with and without surgical stabilization. Classically related to anterior shoulder instability, the incidence and rates of arthritic progression may vary widely. Radiographic arthritic changes may be present in up to two-thirds of patients after primary Bankart repair and 30% after Latarjet procedure, with increasing rates associated with recurrent dislocation history, prominent implant position, non-anatomic reconstruction, and/or lateralized bone graft placement. However, the presence radiographic arthrosis does not predict poor patient-reported function. After exhausting conservative measures, both joint-preserving and arthroplasty surgical options may be considered depending on a combination of patient-specific and anatomic factors. Arthroscopic procedures are optimally indicated for individuals with focal disease and may yield superior symptomatic relief when combined with treatment of combined shoulder pathology. For more advanced secondary arthropathy, total shoulder arthroplasty remains the most reliable option, although the clinical outcomes, wear characteristics, and implant survivorship remains a concern among active, young patients.
Keywords: Arthropathy; Dislocation; Glenohumeral; Instability; Latarjet.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest or relevant financial disclosures related the content of this manuscript. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the United States government. The authors are employees of the United States government.
Figures
References
-
- Owens BD, Dawson L, Burks R, Cameron KL. Incidence of shoulder dislocation in the United States military: demographic considerations from a high-risk population. J Bone Joint Surg Am. 2009;91:791–796. - PubMed
-
- Owens BD, Duffey ML, Nelson BJ, DeBerardino TM, Taylor DC, Mountcastle SB. The incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007;35:1168–1173. - PubMed
-
- Harryman DT, Sidles JA, Harris SL, Matsen FA. The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am. 1992;74:53–66. - PubMed
-
- Krøner K, Lind T, Jensen J. The epidemiology of shoulder dislocations. Arch Orthop Trauma Surg. 1989;108:288–290. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
