

Patterns of Care and Outcomes in Cardiovascular Disease After Kidney Transplantation in the United States
- PMID: 28361110
- PMCID: PMC5367743
- DOI: 10.1097/TXD.0000000000000640
Patterns of Care and Outcomes in Cardiovascular Disease After Kidney Transplantation in the United States
Abstract
Background: Cardiovascular disease (CVD) is an important driver of mortality after kidney transplantation. Its broader impact on posttransplant health care utilization in US hospitals is unknown.
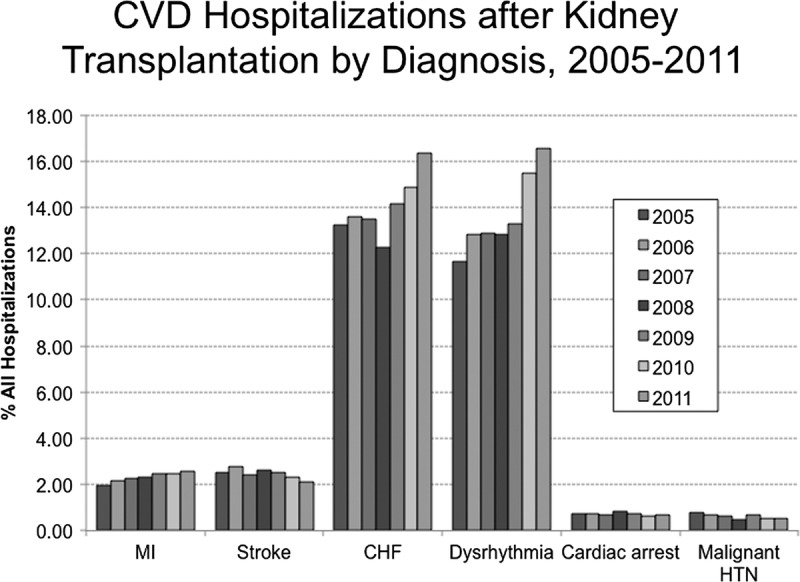
Methods: We used administrative claims data from the Nationwide Inpatient Sample and the American Hospital Association Annual Survey to identify hospitalizations for kidney transplant patients with a cardiovascular diagnosis from 2005 to 2011. CVD hospitalizations were stratified by transplant hospital status to characterize patterns in inpatient health care utilization and outcomes. Based on these analyses, the domestic burden of treatment for posttransplant CVD (myocardial infarction, stroke, congestive heart failure, dysrhythmia, cardiac arrest, malignant hypertension) was estimated.
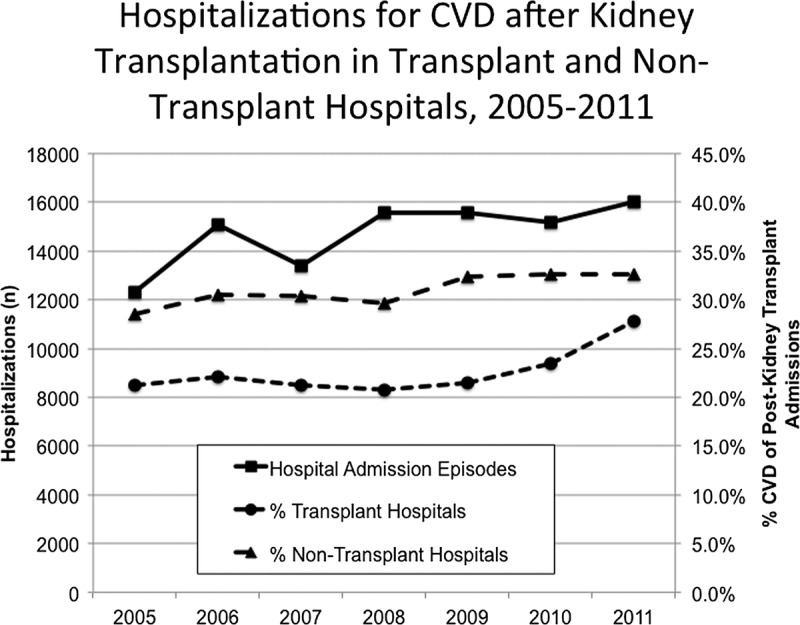
Results: The total domestic burden of post-kidney transplant hospitalization between 2005 and 2011 is estimated at 389 138 of which 26.5% of episodes were related to CVD (n = 103 118). CVD was responsible for a growing proportion of post-transplant hospitalizations over time (24.4%-30.4%, P < 0.001). Compared with nontransplant hospitals, transplant hospitals had similar length of stay (median length of stay, 3.7 days), higher median costs per hospitalization (US $10 364 vs US $8606, overall US $9324), and lower adjusted mortality (3.2% vs 3.9%, overall 3.6%; P = 0.003).
Conclusions: Inpatient CVD care is increasing over time for kidney transplant patients, accounting for 30% of all post-transplant hospitalizations. Variation exists in the inpatient care, outcomes, and costs between by hospital type. Further studies are needed to better understand the mechanisms behind these phenomena.
Conflict of interest statement
The authors have no funding or conflicts of interest.
Figures
References
-
- Port FK, Wolfe RA, Mauger EA, et al. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993;270:1339–1343. - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. - PubMed
-
- Stoumpos S, Jardine AG, Mark PB. Cardiovascular morbidity and mortality after kidney transplantation. Transpl Int. 2015;28:10–21. - PubMed
-
- Liefeldt L, Budde K. Risk factors for cardiovascular disease in renal transplant recipients and strategies to minimize risk. Transpl Int. 2010;23:1191–1204. - PubMed
-
- Lam NN, Kim SJ, Knoll GA, et al. The risk of cardiovascular disease is not increasing over time despite aging and higher comorbidity burden of kidney transplant recipients. Transplantation. 2016. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
