

Socioeconomic Factors Explain Racial Disparities in Invasive Community-Associated Methicillin-Resistant Staphylococcus aureus Disease Rates
- PMID: 28362911
- PMCID: PMC5656382
- DOI: 10.1093/cid/ciw808
Socioeconomic Factors Explain Racial Disparities in Invasive Community-Associated Methicillin-Resistant Staphylococcus aureus Disease Rates
Abstract
Background: Invasive community-associated methicillin-resistant Staphylococcus aureus (MRSA) incidence in the United States is higher among black persons than white persons. We explored the extent to which socioeconomic factors might explain this racial disparity.
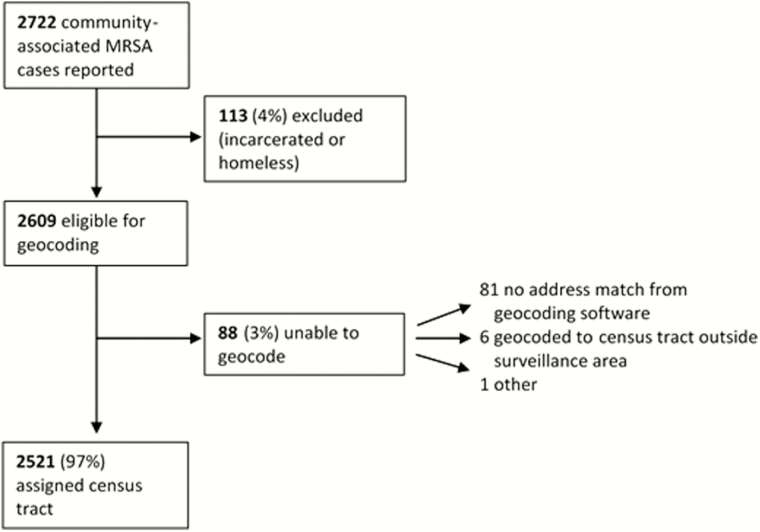
Methods: A retrospective cohort was based on the Centers for Disease Control and Prevention's Emerging Infections Program surveillance data for invasive community-associated MRSA cases (isolated from a normally sterile site of an outpatient or on hospital admission day ≤3 in a patient without specified major healthcare exposures) from 2009 to 2011 in 33 counties of 9 states. We used generalized estimating equations to determine census tract-level factors associated with differences in MRSA incidence and inverse odds ratio-weighted mediation analysis to determine the proportion of racial disparity mediated by socioeconomic factors.
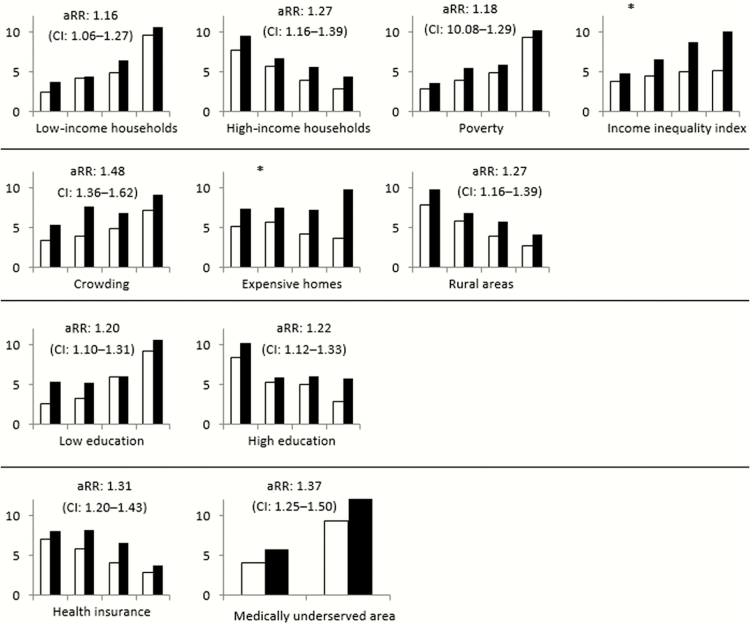
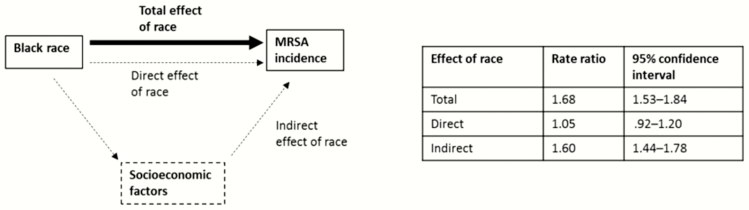
Results: Annual invasive community-associated MRSA incidence was 4.59 per 100000 among whites and 7.60 per 100000 among blacks (rate ratio [RR], 1.66; 95% confidence interval [CI], 1.52-1.80). In the mediation analysis, after accounting for census tract-level measures of federally designated medically underserved areas, education, income, housing value, and rural status, 91% of the original racial disparity was explained; no significant association of black race with community-associated MRSA remained (RR, 1.05; 95% CI, .92-1.20).
Conclusions: The racial disparity in invasive community-associated MRSA rates was largely explained by socioeconomic factors. The specific factors that underlie the association between census tract-level socioeconomic measures and MRSA incidence, which may include modifiable social (eg, poverty, crowding) and biological factors (not explored in this analysis), should be elucidated to define strategies for reducing racial disparities in community-associated MRSA rates.
Keywords: antibiotic resistance; methicillin-resistant Staphylococcus aureus; racial disparities; social determinants of health.
Published by Oxford University Press for the Infectious Diseases Society of America 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- National Nosocomial Infections Surveillance System. National nosocomial infections surveillance (NNIS) system report, data summary from 1992 to June 2002, issued August 2002. Am J Infect Control 2002; 30:458–75. - PubMed
-
- Brumfitt W, Hamilton-Miller J. Methicillin-resistant Staphylococcus aureus. N Engl J Med 1989; 320:1188–96. - PubMed
-
- Jorgensen JH. Laboratory and epidemiologic experience with methicillin-resistant Staphylococcus aureus in the USA. Eur J Clin Microbiol 1986; 5:693–6. - PubMed
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013 Available at: http://www.cdc.gov/drugresistance/threat-report-2013/ Accessed 16 June 2016.
-
- Healthcare Infection Control Practices Advisory Committee (HICPAC). 2007 guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings Available at: http://www.cdc.gov/hicpac/2007IP/2007isolationPrecautions.html Accessed 2 February 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
