

Geographic Differences in Temporal Incidence Trends of Hepatitis C Virus Infection Among People Who Inject Drugs: The InC3 Collaboration
- PMID: 28362947
- PMCID: PMC5439493
- DOI: 10.1093/cid/ciw869
Geographic Differences in Temporal Incidence Trends of Hepatitis C Virus Infection Among People Who Inject Drugs: The InC3 Collaboration
Erratum in
-
Erratum.Clin Infect Dis. 2017 Aug 15;65(4):706-707. doi: 10.1093/cid/cix450. Clin Infect Dis. 2017. PMID: 29017273 Free PMC article. No abstract available.
Abstract
Background: We determined temporal trends (1985-2011) in hepatitis C virus (HCV) incidence and associated behavioral exposures for people who inject drugs (PWID) from the United States (Boston, Baltimore, and San Francisco), Canada (Montreal), the Netherlands (Amsterdam), and Australia (Sydney and Melbourne).
Methods: Using population-based cohort data from HCV-negative PWID, we calculated overall and within-city HCV incidence trends, HCV rates by study enrollment period (1985-2011), and temporal trends in exposure behaviors. Poisson regression models estimated trends in HCV incidence over calendar-time. Survival models identified risk factors for HCV incidence across cities and estimated independent effects of city and calendar period on HCV infection risk.
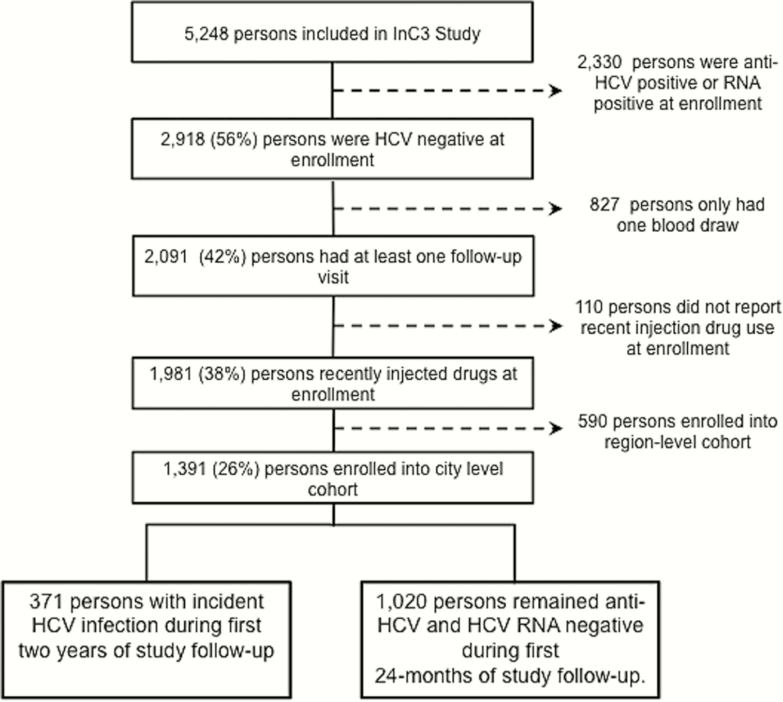
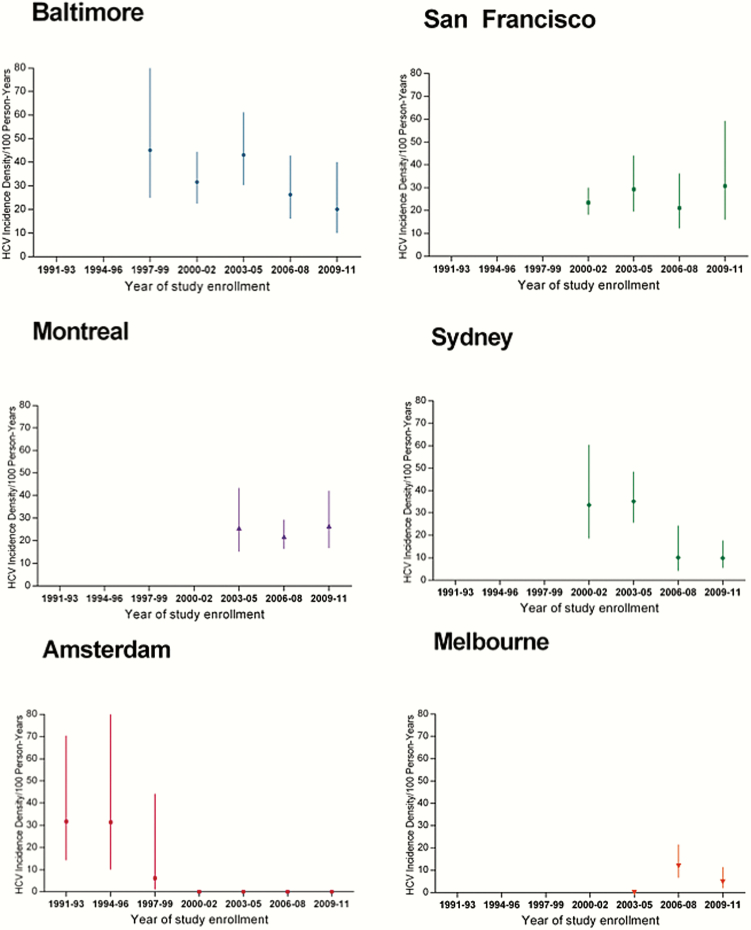
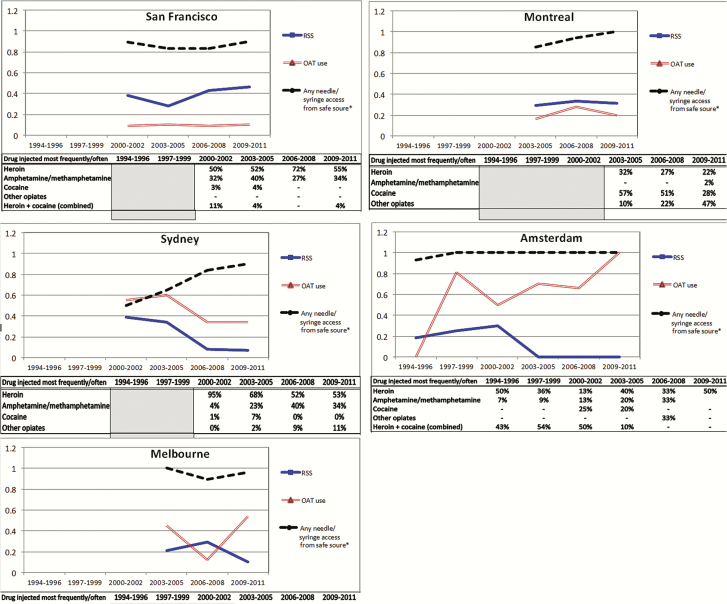
Results: Among 1391 initially HCV-negative participants followed prospectively (1644.5 person-years of observation [PYO]), 371 HCV incident infections resulted in an overall incidence of 22.6 per 100 PYO (95% confidence interval [CI], 20.4-25.0). Incidence was highest and remained elevated in Baltimore (32.6/100 PYO), San Francisco (24.7/100 PYO), and Montreal (23.5/100 PYO), lowest in Melbourne and Amsterdam (7.5/100 PYO and 13.1/100 PYO, respectively), and moderate (21.4/100 PYO) in Sydney. Higher rates of syringe and equipment sharing and lower prevalence of opioid agonist therapy were associated with HCV incidence in cities with the highest incidence. Risk for infection dropped by 18% for every 3-year increase in calendar-time (adjusted hazard ratio, 0.8 [95% CI, .8-.9]) in the multivariable model.
Conclusions: Differences in prevention strategies and injecting contexts may explain the ongoing high HCV incidence in these North American cities and emphasize the need for scale-up of opioid agonist therapy and increased coverage of needle and syringe programs in North America.
Keywords: epidemiology; harm reduction strategies.; hepatitis C virus (HCV); incidence trends; people who inject drugs.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Aceijas C, Rhodes T. Global estimates of prevalence of HCV infection among injecting drug users. Int J Drug Policy 2007; 18:352–8. - PubMed
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013; 57:1333–42. - PubMed
-
- Patti AM, Santi AL, Pompa MG, et al. Viral hepatitis and drugs: a continuing problem. Int J Epidemiol 1993; 22:135–9. - PubMed
-
- Hagan H, Des Jarlais DC, Stern R, et al. HCV synthesis project: preliminary analyses of HCV prevalence in relation to age and duration of injection. Int J Drug Policy 2007; 18:341–51. - PubMed
-
- Sievert W, Altraif I, Razavi HA, et al. A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver Int 2011; 31(suppl 2):61–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
