

ACC/AHA guidelines superior to ESC/EAS guidelines for primary prevention with statins in non-diabetic Europeans: the Copenhagen General Population Study
- PMID: 28363217
- PMCID: PMC5837499
- DOI: 10.1093/eurheartj/ehw426
ACC/AHA guidelines superior to ESC/EAS guidelines for primary prevention with statins in non-diabetic Europeans: the Copenhagen General Population Study
Abstract
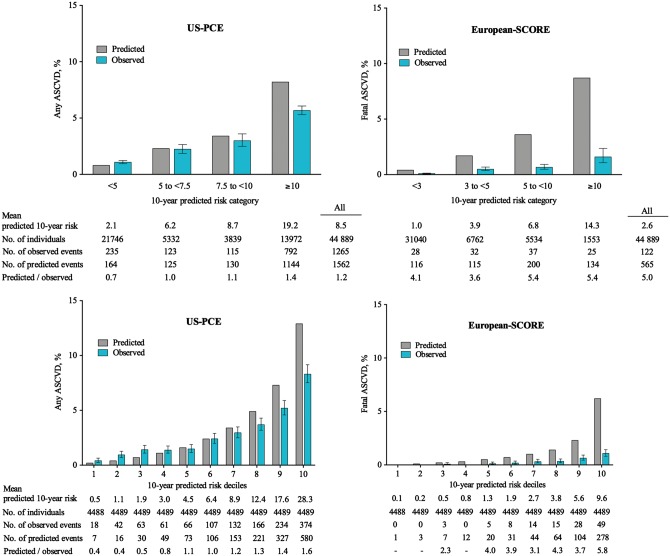
Aim: We compared the 2013 American College of Cardiology/American Heart Association (ACC/AHA) and the 2016 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines on prevention of atherosclerotic cardiovascular disease (ASCVD) using different risk prediction models [US Pooled Cohort Equations (US-PCE for any ASCVD) and European Systematic COronary Risk Evaluation system (European-SCORE for fatal ASCVD)] and different statin eligibility criteria.
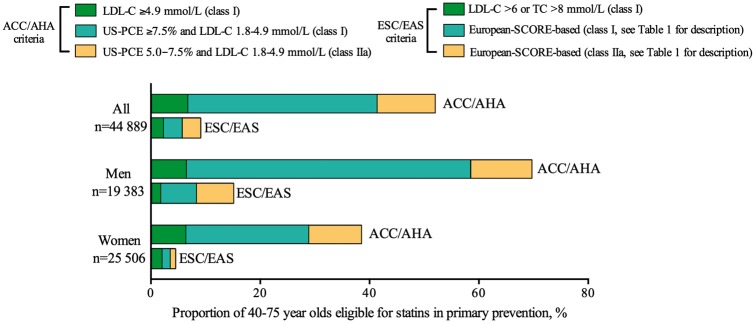
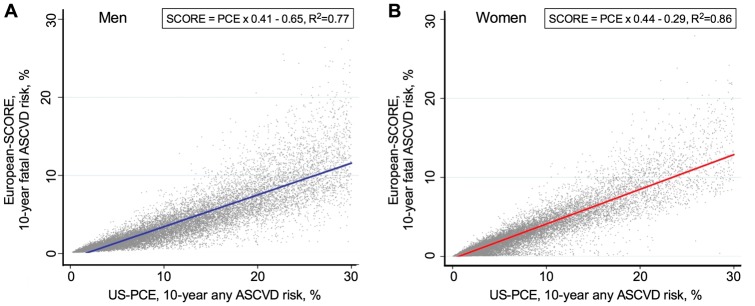
Methods and results: We examined 44 889 individuals aged 40-75 recruited in 2003-09 in the Copenhagen General Population Study, all free of ASCVD, diabetes, and statin use at baseline. We detected 2217 any ASCVD events and 199 fatal ASCVD events through 2014. The predicted-to-observed event ratio was 1.2 using US-PCE for any ASCVD and 5.0 using European-SCORE for fatal ASCVD. The US-PCE, but not the European-SCORE, was well-calibrated around decision thresholds for statin therapy. For a Class I recommendation, 42% of individuals qualified for statins using the ACC/AHA guidelines vs. 6% with the ESC/EAS guidelines. Using ACC/AHA- vs. ESC/EAS-defined statin eligibility led to a substantial gain in sensitivity (+62% for any ASCVD and +76% for fatal ASCVD) with a smaller loss in specificity (-35% for any ASCVD and -36% for fatal ASCVD). Similar differences between the ACC/AHA and ESC/EAS guidelines were found for men and women separately, and for Class IIa recommendations. The sensitivity and specificity of a US-PCE risk of 5% were similar to those of a European-SCORE risk of 1.4%, whereas a US-PCE risk of 7.5% was similar to a European-SCORE risk of 2.4%.
Conclusions: The ACC/AHA guidelines were superior to the ESC/EAS guidelines for primary prevention of ASCVD, that is, for accurately assigning statin therapy to those who would benefit.
Keywords: Atherosclerosis; Guideline; Lipids; Lipoproteins; Myocardial infarction; Stroke.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology
Figures
Comment in
-
Time to change the SCORE?Eur Heart J. 2017 Feb 21;38(8):595-597. doi: 10.1093/eurheartj/ehw428. Eur Heart J. 2017. PMID: 28363220 No abstract available.
References
-
- Murray CJ, Lopez AD.. Measuring the global burden of disease. N Engl J Med 2013;369:448–457. - PubMed
-
- Laslett LJ, Alagona P Jr, Clark BA III, Drozda JP Jr, Saldivar F, Wilson SR, Poe C, Hart M.. The worldwide environment of cardiovascular disease: prevalence, diagnosis, therapy, and policy issues: a report from the American College of Cardiology. J Am Coll Cardiol 2012;60:S1–S49. - PubMed
-
- Dudas K, Lappas G, Stewart S, Rosengren A.. Trends in out-of-hospital deaths due to coronary heart disease in Sweden (1991 to 2006). Circulation 2011;123:46–52. - PubMed
-
- Capewell S, O’Flaherty M.. Rapid mortality falls after risk-factor changes in populations. Lancet 2011;378:752–753. - PubMed
-
- Jørgensen T, Capewell S, Prescott E, Allender S, Sans S, Zdrojewski T, De Bacquer D, de Sutter J, Franco OH, Løgstrup S, Volpe M, Malyutina S, Marques-Vidal P, Reiner Z, Tell GS, Verschuren WM, Vanuzzo D, PEP Section of EACPR. Population-level changes to promote cardiovascular health. Eur J Prev Cardiol 2013;20:409–421. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
