

Safety, tolerability, pharmacokinetics, and activity of the novel long-acting antimalarial DSM265: a two-part first-in-human phase 1a/1b randomised study
- PMID: 28363636
- PMCID: PMC5446412
- DOI: 10.1016/S1473-3099(17)30171-8
Safety, tolerability, pharmacokinetics, and activity of the novel long-acting antimalarial DSM265: a two-part first-in-human phase 1a/1b randomised study
Abstract
Background: DSM265 is a novel antimalarial that inhibits plasmodial dihydroorotate dehydrogenase, an enzyme essential for pyrimidine biosynthesis. We investigated the safety, tolerability, and pharmacokinetics of DSM265, and tested its antimalarial activity.
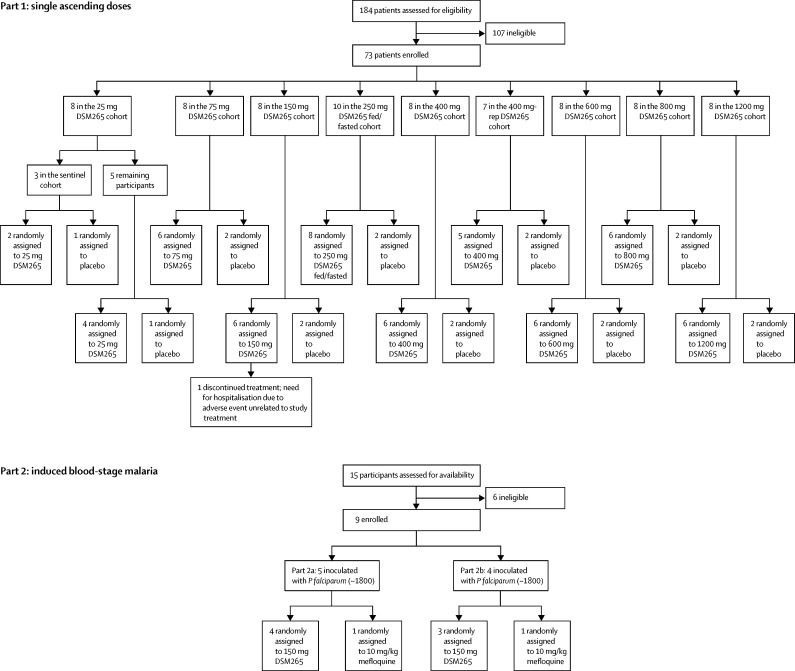
Methods: Healthy participants aged 18-55 years were enrolled in a two-part study: part 1, a single ascending dose (25-1200 mg), double-blind, randomised, placebo-controlled study, and part 2, an open-label, randomised, active-comparator controlled study, in which participants were inoculated with Plasmodium falciparum induced blood-stage malaria (IBSM) and treated with DSM265 (150 mg) or mefloquine (10 mg/kg). Primary endpoints were DSM265 safety, tolerability, and pharmacokinetics. Randomisation lists were created using a validated, automated system. Both parts were registered with the Australian New Zealand Clinical Trials Registry, number ACTRN12613000522718 (part 1) and number ACTRN12613000527763 (part 2).
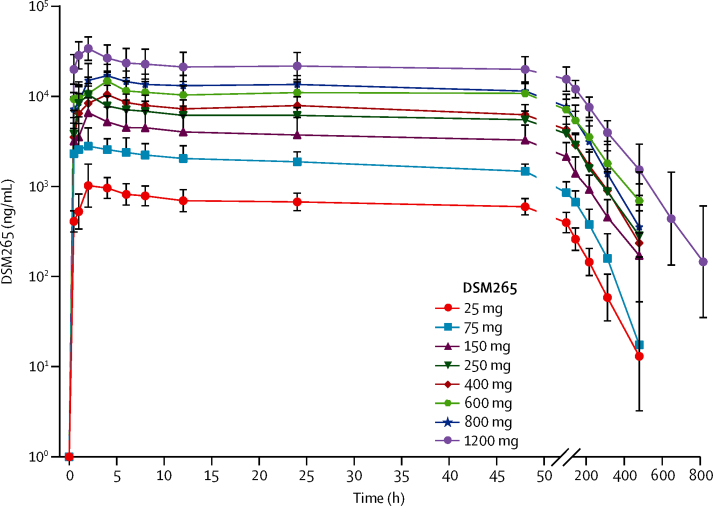
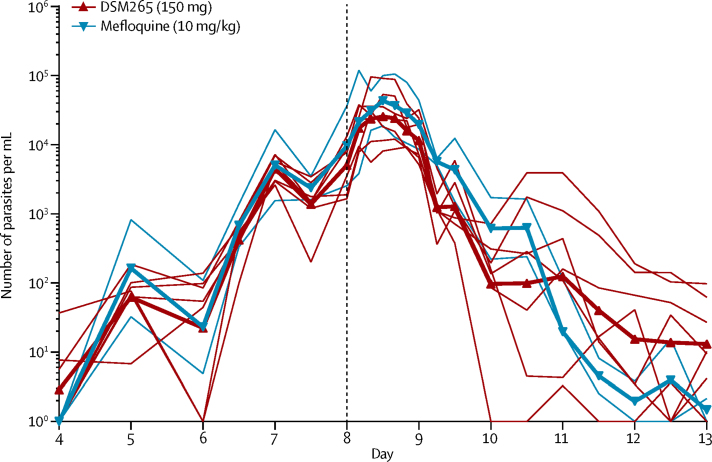
Findings: In part 1, 73 participants were enrolled between April 12, 2013, and July 14, 2015 (DSM265, n=55; placebo, n=18). In part 2, nine participants were enrolled between Sept 30 and Nov 25, 2013 (150 mg DSM265, n=7; 10 mg/kg mefloquine, n=2). In part 1, 117 adverse events were reported; no drug-related serious or severe events were reported. The most common drug-related adverse event was headache. The mean DSM265 peak plasma concentration (Cmax) ranged between 1310 ng/mL and 34 800 ng/mL and was reached in a median time (tmax) between 1·5 h and 4 h, with a mean elimination half-life between 86 h and 118 h. In part 2, the log10 parasite reduction ratio at 48 h in the DSM265 (150 mg) group was 1·55 (95% CI 1·42-1·67) and in the mefloquine (10 mg/kg) group was 2·34 (2·17-2·52), corresponding to a parasite clearance half-life of 9·4 h (8·7-10·2) and 6·2 h (5·7-6·7), respectively. The median minimum inhibitory concentration of DSM265 in blood was estimated as 1040 ng/mL (range 552-1500), resulting in a predicted single efficacious dose of 340 mg. Parasite clearance was significantly faster in participants who received mefloquine than in participants who received DSM265 (p<0·0001).
Interpretation: The good safety profile, long elimination half-life, and antimalarial effect of DSM265 supports its development as a partner drug in a single-dose antimalarial combination treatment.
Funding: Wellcome Trust, UK Department for International Development, Global Health Innovative Technology Fund, Bill & Melinda Gates Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Investment in antimalarial drug development is bearing fruit.Lancet Infect Dis. 2017 Jun;17(6):568-570. doi: 10.1016/S1473-3099(17)30172-X. Epub 2017 Mar 28. Lancet Infect Dis. 2017. PMID: 28363638 No abstract available.
References
-
- WHO World Malaria Report 2016. http://www.who.int/malaria/media/world-malaria-report-2016/en/ (accessed Dec 15, 2016).
-
- WHO . Artemisinin and artemisinin-based combination therapy resistance. Status report. World Health Organization; Geneva: 2016.
-
- Spring MD, Lin JT, Manning JE. Dihydroartemisinin-piperaquine failure associated with a triple mutant including kelch13 C580Y in Cambodia: an observational cohort study. Lancet Infect Dis. 2015;15:683–691. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
