

Evidence of potential bias in a comparison of β blockers and calcium channel blockers in patients with chronic obstructive pulmonary disease and acute coronary syndrome: results of a multinational study
- PMID: 28363921
- PMCID: PMC5387948
- DOI: 10.1136/bmjopen-2016-012997
Evidence of potential bias in a comparison of β blockers and calcium channel blockers in patients with chronic obstructive pulmonary disease and acute coronary syndrome: results of a multinational study
Abstract
Objectives: A number of observational studies have reported that, in patients with chronic obstructive pulmonary disease (COPD), β blockers (BBs) decrease risk of mortality and COPD exacerbations. To address important methodological concerns of these studies, we compared the effectiveness and safety of cardioselective BBs versus non-dihydropyridine calcium channel blockers (non-DHP CCBs) in patients with COPD and acute coronary syndromes (ACS) using a propensity score (PS)-matched, active comparator, new user design. We also assessed for potential unmeasured confounding by examining a short-term COPD hospitalisation outcome.
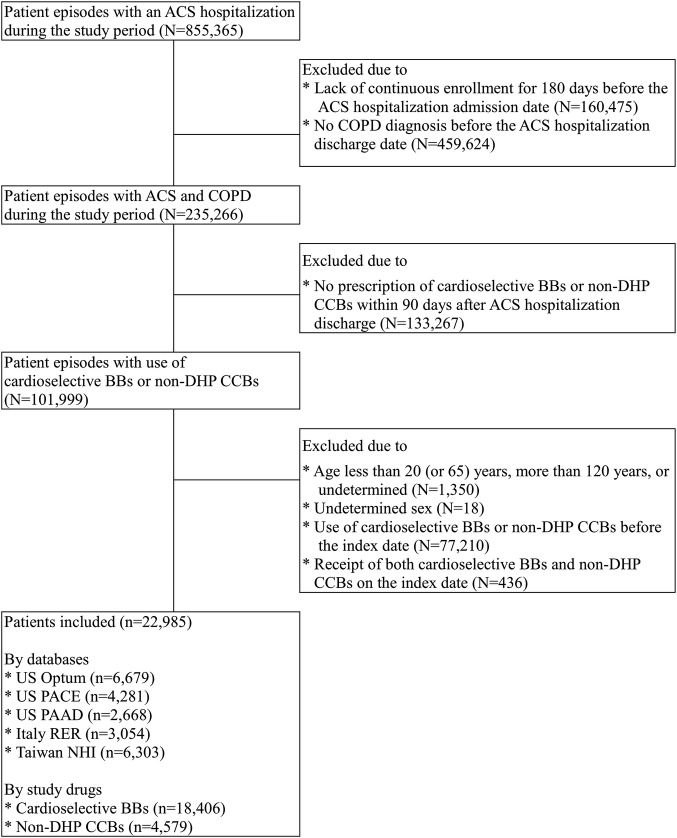
Setting and participants: We identified 22 985 patients with COPD and ACS starting cardioselective BBs or non-DHP CCBs across 5 claims databases from the USA, Italy and Taiwan.
Primary and secondary outcome measures: Stratified Cox regression models were used to estimate HRs for mortality, cardiovascular (CV) hospitalisations and COPD hospitalisations in each database after variable-ratio PS matching. Results were combined with random-effects meta-analyses.
Results: Cardioselective BBs were not associated with reduced risk of mortality (HR, 0.90; 95% CI 0.78 to 1.02) or CV hospitalisations (HR, 1.06; 95% CI 0.91 to 1.23), although statistical heterogeneity was observed across databases. In contrast, a consistent, inverse association for COPD hospitalisations was identified across databases (HR, 0.54; 95% CI 0.47 to 0.61), which persisted even within the first 30 days of follow-up (HR, 0.55; 95% CI 0.37 to 0.82). Results were similar across a variety of sensitivity analyses, including PS trimming, high dimensional-PS matching and restricting to high-risk patients.
Conclusions: This multinational study found a large inverse association between cardioselective BBs and short-term COPD hospitalisations. The persistence of this bias despite state-of-the-art pharmacoepidemiologic methods calls into question the ability of claims data to address confounding in studies of BBs in patients with COPD.
Keywords: COPD hospitalizations; acute coronary syndromes; cardioselective β-blockers; chronic obstructive pulmonary disease; mortality; unmeasured confounding.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures
Similar articles
-
Use of cardioselective β-blockers and overall death and cardiovascular outcomes in patients with COPD: a population-based cohort study.Eur J Clin Pharmacol. 2016 Oct;72(10):1265-1273. doi: 10.1007/s00228-016-2097-y. Epub 2016 Jul 22. Eur J Clin Pharmacol. 2016. PMID: 27444174
-
Under-utilisation of β-blockers in patients with acute coronary syndrome and comorbid chronic obstructive pulmonary disease.Intern Med J. 2018 Aug;48(8):931-936. doi: 10.1111/imj.13795. Intern Med J. 2018. PMID: 29573074
-
Outcomes in patients hospitalized for heart failure and chronic obstructive pulmonary disease: differences in clinical profile and treatment between 2002 and 2009.Eur J Heart Fail. 2016 Jul;18(7):840-8. doi: 10.1002/ejhf.519. Epub 2016 Apr 21. Eur J Heart Fail. 2016. PMID: 27098360
-
Association of β-blocker use with survival and pulmonary function in patients with chronic obstructive pulmonary and cardiovascular disease: a systematic review and meta-analysis.Eur Heart J. 2020 Dec 7;41(46):4415-4422. doi: 10.1093/eurheartj/ehaa793. Eur Heart J. 2020. PMID: 33211823 Free PMC article.
-
Beta-Blockers in COPD: A Methodological Review of the Observational Studies.COPD. 2018 Oct;15(5):520-525. doi: 10.1080/15412555.2018.1554637. COPD. 2018. PMID: 30822238 Review.
Cited by
-
Machine learning for improving high-dimensional proxy confounder adjustment in healthcare database studies: An overview of the current literature.Pharmacoepidemiol Drug Saf. 2022 Sep;31(9):932-943. doi: 10.1002/pds.5500. Epub 2022 Jul 5. Pharmacoepidemiol Drug Saf. 2022. PMID: 35729705 Free PMC article. Review.
-
Bias in pharmacoepidemiologic studies using secondary health care databases: a scoping review.BMC Med Res Methodol. 2019 Mar 11;19(1):53. doi: 10.1186/s12874-019-0695-y. BMC Med Res Methodol. 2019. PMID: 30871502 Free PMC article.
-
β-blockers after acute myocardial infarction in patients with chronic obstructive pulmonary disease: A nationwide population-based observational study.PLoS One. 2019 Mar 5;14(3):e0213187. doi: 10.1371/journal.pone.0213187. eCollection 2019. PLoS One. 2019. PMID: 30835781 Free PMC article.
References
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary diseases 2013. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2013_Feb20.pdf (accessed 5 Jul 2014).
-
- World Health Organization. World Health Statistics 2008. http://www.who.int/whosis/whostat/2008/en/ (accessed 5 Jul 2014).
-
- Sin DD, Man SFP. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation 2003;107:1514–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical