

How common and frequent is heterosexual anal intercourse among South Africans? A systematic review and meta-analysis
- PMID: 28364565
- PMCID: PMC5461120
- DOI: 10.7448/IAS.20.1.21162
How common and frequent is heterosexual anal intercourse among South Africans? A systematic review and meta-analysis
Abstract
Background: HIV is transmitted more effectively during anal intercourse (AI) than vaginal intercourse (VI). However, patterns of heterosexual AI practice and its contribution to South Africa's generalized epidemic remain unclear. We aimed to determine how common and frequent heterosexual AI is in South Africa.
Methods: We searched for studies reporting the proportion practising heterosexual AI (prevalence) and/or the number of AI and unprotected AI (UAI) acts (frequency) in South Africa from 1990 to 2015. Stratified random-effects meta-analysis by sub-groups was used to produce pooled estimates and assess the influence of participant and study characteristics on AI prevalence. We also estimated the fraction of all sex acts which were AI or UAI and compared condom use during VI and AI.
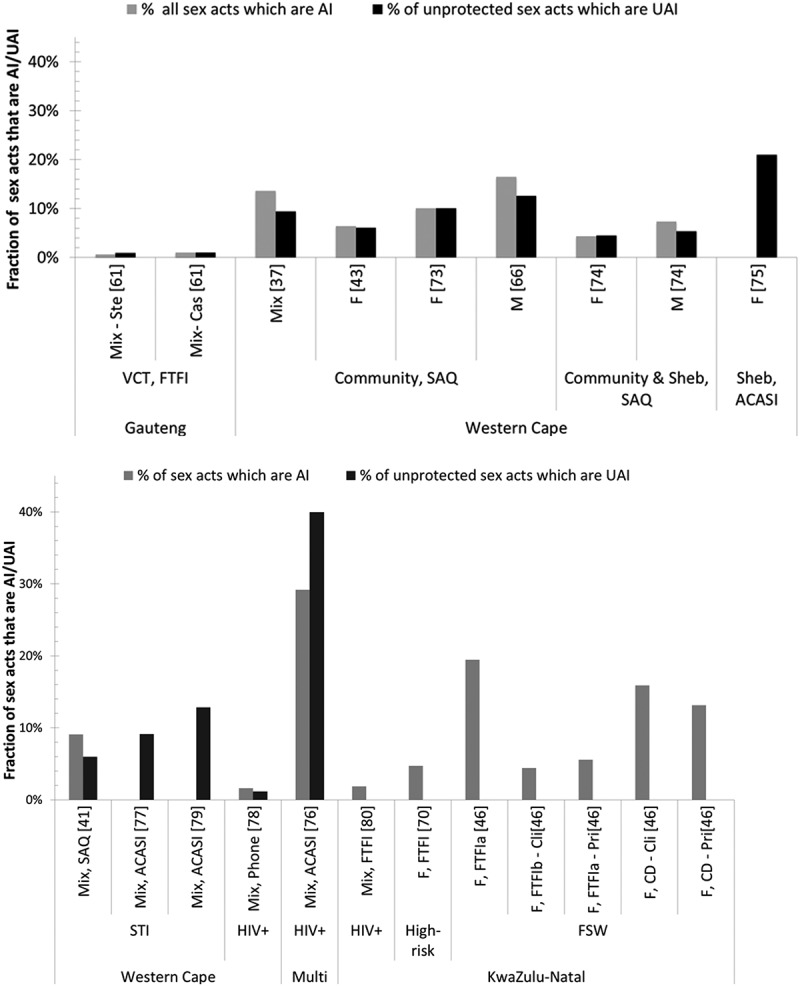
Results: Of 41 included studies, 31 reported on AI prevalence and 14 on frequency, over various recall periods. AI prevalence was high across different recall periods for sexually active general-risk populations (e.g. lifetime = 18.4% [95%CI:9.4-27.5%], three-month = 20.3% [6.1-34.7%]), but tended to be even higher in higher-risk populations such as STI patients and female sex workers (e.g. lifetime = 23.2% [0.0-47.4%], recall period not stated = 40.1% [36.2-44.0%]). Prevalence was higher in studies using more confidential interview methods. Among general and higher-risk populations, 1.2-40.0% and 0.7-21.0% of all unprotected sex acts were UAI, respectively. AI acts were as likely to be condom protected as vaginal acts.
Conclusion: Reported heterosexual AI is common but variable among South Africans. Nationally and regionally representative sexual behaviour studies that use standardized recall periods and confidential interview methods, to aid comparison across studies and minimize reporting bias, are needed. Such data could be used to estimate the extent to which AI contributes to South Africa's HIV epidemic.
Keywords: Anal intercourse; South Africa; heterosexual; sexual behaviour.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
