

Marijuana and acute health care contacts in Colorado
- PMID: 28365373
- PMCID: PMC5623152
- DOI: 10.1016/j.ypmed.2017.03.022
Marijuana and acute health care contacts in Colorado
Abstract
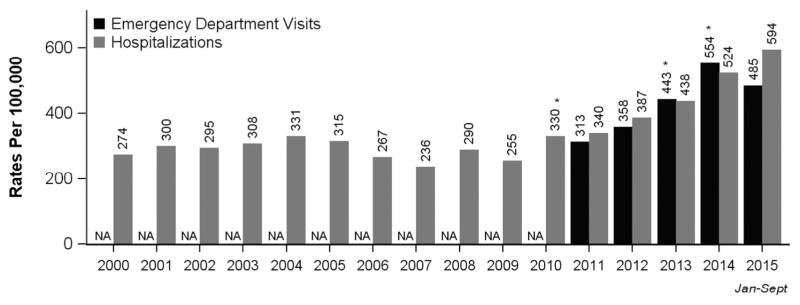
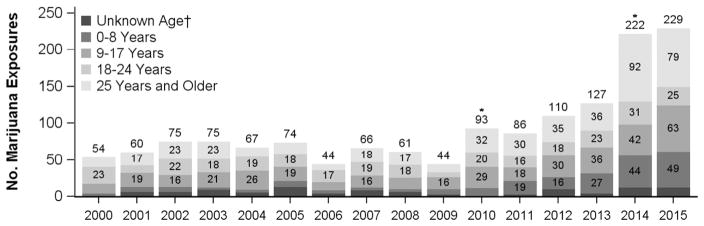
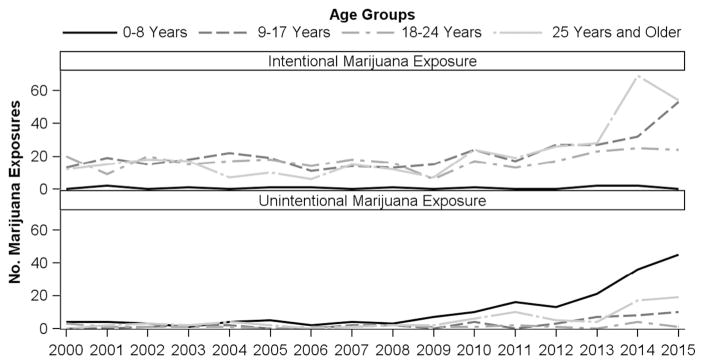
Over 22 million Americans are current users of marijuana; half of US states allow medical marijuana, and several allow recreational marijuana. The objective of this study was to evaluate the impact marijuana has on hospitalizations, emergency department (ED) visits, and regional poison center (RPC) calls in Colorado, a medical and recreational marijuana state. This is a retrospective review using Colorado Hospital Association hospitalizations and ED visits with marijuana-related billing codes, and RPC marijuana exposure calls. Legalization of marijuana in Colorado has been associated with an increase in hospitalizations, ED visits, and RPC calls linked with marijuana exposure. From 2000 to 2015, hospitalization rates with marijuana-related billing codes increased from 274 to 593 per 100,000 hospitalizations in 2015. Overall, the prevalence of mental illness among ED visits with marijuana-related codes was five-fold higher (5.07, 95% CI: 5.0, 5.1) than the prevalence of mental illness without marijuana-related codes. RPC calls remained constant from 2000 through 2009. However, in 2010, after local medical marijuana policy liberalization, the number of marijuana exposure calls significantly increased from 42 to 93; in 2014, after recreational legalization, calls significantly increased by 79.7%, from 123 to 221 (p<0.0001). The age group <17years old also had an increase in calls after 2014. As more states legalize marijuana, it is important to address public education and youth prevention, and understand the impact on mental health disorders. Improvements in data collection and surveillance methods are needed to more accurately evaluate the public health impact of marijuana legalization.
Keywords: Cannabis; Colorado; Emergency department; Emergency room; Hospitalizations; Legalization; Marijuana; Poison center.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Wang has a Colorado Department of Public Health and Environment (CDPHE) Grant evaluating cannabidiol in pediatric epilepsy patients. He also receives royalties from UpToDate on related subject matter. Dr. Monte receives support from NIH 1 K23 GM110516 and NIH CTSI UL1 TR001082. Dr. Monte is partially funded by a grant through the CDPHE to study the public health effects of cannabis edible products in Colorado. Dr. Monte has a patent pending for a synthetic cannabinoid clinical assay and has been award funding through the Department of Defense for examination of patterns of use of synthetic cannabinoids and assay development. All authors participate on the CDPHE Retail Marijuana Public Health Advisory Committee.
Figures
References
-
- Aspis I, Feingold D, Weiser M, et al. Cannabis use and mental health-related quality of life among individuals with depressive disorders. Psychiatry Res. 2015;230:341–349. http://dx.doi.org/10.1016/j.psychres.2015.09.014. - DOI - PubMed
-
- Center for Behavioral Health Statistics and Quality. 2015 National Survey on Drug Use and Health: Detailed Tables. Substance Abuse and Mental Health Services Administration; Rockville, MD: 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
