

Prognostic Significance of Interleukin-34 (IL-34) in Patients With Chronic Heart Failure With or Without Renal Insufficiency
- PMID: 28365566
- PMCID: PMC5533008
- DOI: 10.1161/JAHA.116.004911
Prognostic Significance of Interleukin-34 (IL-34) in Patients With Chronic Heart Failure With or Without Renal Insufficiency
Abstract
Background: Renal dysfunction, commonly associated with cardiac dysfunction, has predictive value for adverse long-term outcomes in heart failure (HF). We previously identified a novel renal biomarker, interleukin-34 (IL-34), elevated in HF patients and associated with kidney dysfunction and coronary artery disease during HF. However, the prognostic value of IL-34 in HF remains unclear, so that the present study aimed to determine it.
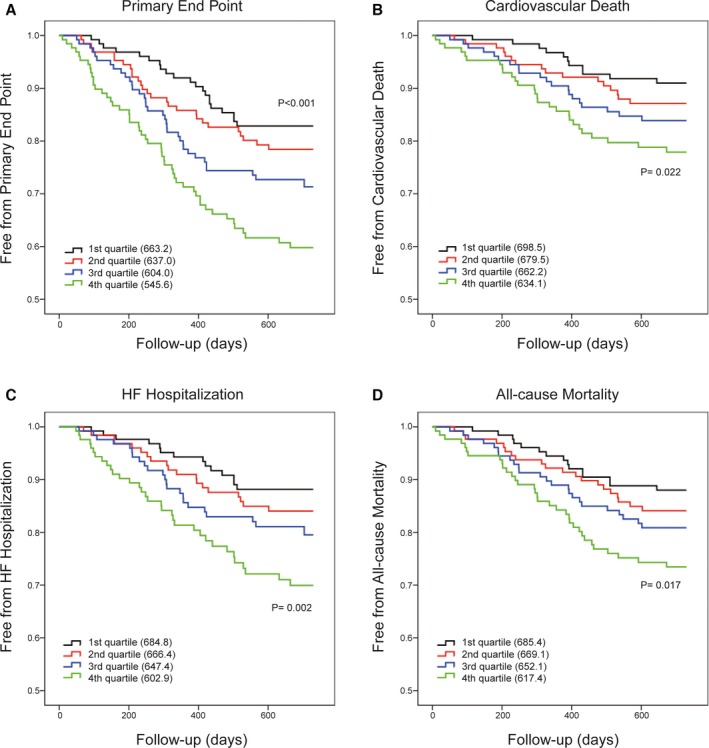
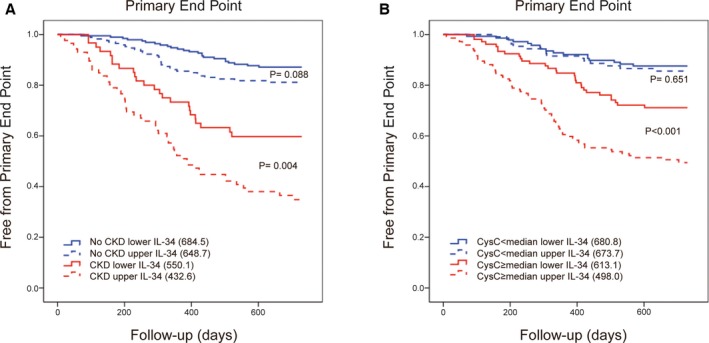
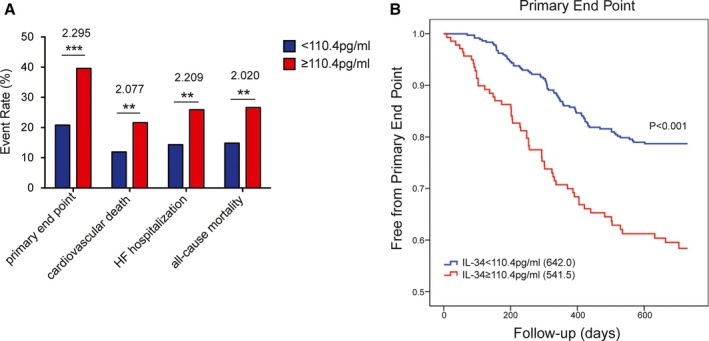
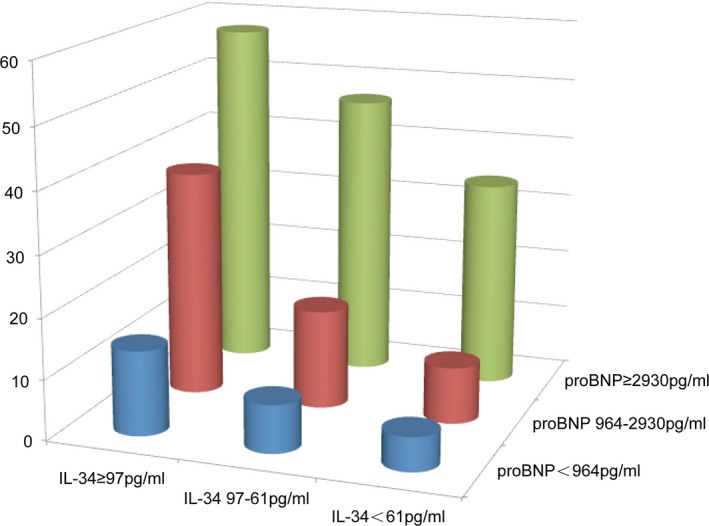
Methods and results: This prospective, observational study included 510 consecutive HF patients with their serum IL-34 as well as other variables measured at baseline, and they were followed up for 2 years. The primary end point was a composite of cardiovascular death or a first HF hospitalization, with cardiovascular death, HF hospitalization, and all-cause mortality as secondary outcomes. There was a significant and gradual increase in risk as IL-34 increased, determined by log-rank tests with Kaplan-Meier curves. Serum IL-34 was also a significant prognostic predictor of the primary end point (1.301 [1.115-1.518]; P=0.001), cardiovascular death (1.347 [1.096-1.655]; P=0.005), HF hospitalization (1.234 [1.018-1.494]; P=0.032), and all-cause mortality (1.343 [1.115-1.618]; P=0.002) in HF as per SD increase in the log IL-34 level after adjusting for age, sex, traditional risk factors, and N-terminal pro-brain natriuretic peptide. Especially, IL-34 had a more-significant prognostic value in HF patients with kidney impairment than those without.
Conclusions: IL-34 is a significant predictor of cardiovascular death, HF hospitalization, and all-cause mortality in chronic HF, especially when concomitant with renal dysfunction. Serum IL-34 measurement may provide new insights linking kidney impairment to poor HF outcomes beyond other renal markers.
Keywords: heart failure; interleukin‐34; prognosis; renal insufficiency.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Metra M, Cotter G, Gheorghiade M, Dei Cas L, Voors AA. The role of the kidney in heart failure. Eur Heart J. 2012;33:2135–2142. - PubMed
-
- Ather S, Chan W, Bozkurt B, Aguilar D, Ramasubbu K, Zachariah AA, Wehrens XH, Deswal A. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J Am Coll Cardiol. 2012;59:998–1005. - PMC - PubMed
-
- Dries DL, Exner DV, Domanski MJ, Greenberg B, Stevenson LW. The prognostic implications of renal insufficiency in asymptomatic and symptomatic patients with left ventricular systolic dysfunction. J Am Coll Cardiol. 2000;35:681–689. - PubMed
-
- Lin H, Lee E, Hestir K, Leo C, Huang M, Bosch E, Halenbeck R, Wu G, Zhou A, Behrens D, Hollenbaugh D, Linnemann T, Qin M, Wong J, Chu K, Doberstein SK, Williams LT. Discovery of a cytokine and its receptor by functional screening of the extracellular proteome. Science. 2008;320:807–811. - PubMed
-
- Masteller EL, Wong BR. Targeting IL‐34 in chronic inflammation. Drug Discov Today. 2014;19:1212–1216. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
