

Early extubation is associated with reduced length of stay and improved outcomes after elective aortic surgery in the Vascular Quality Initiative
- PMID: 28366307
- PMCID: PMC6114133
- DOI: 10.1016/j.jvs.2016.12.122
Early extubation is associated with reduced length of stay and improved outcomes after elective aortic surgery in the Vascular Quality Initiative
Abstract
Objective: Timing of extubation after open aortic procedures varies across hospitals. This study was designed to examine extubation timing and determine its effect on length of stay (LOS) and respiratory complications after elective open aortic surgery.
Methods: We studied extubation timing for 7171 patients undergoing elective open abdominal aortic aneurysm repair (2687 [37.5%]) or suprainguinal bypass for aortoiliac occlusive disease (4484 [62.5%]) from October 2010 to April 2015 in hospitals participating in the Vascular Quality Initiative (VQI). Our primary outcome was prolonged LOS (>7 days), and the secondary outcome was respiratory complications (pneumonia or reintubation). The association between extubation timing and outcomes was assessed using multivariable logistic regression mixed-effects models that adjusted for confounding factors at the patient and procedure level. A variable importance analysis was conducted using a chi-pie framework to identify factors contributing to the variability of extubation timing.
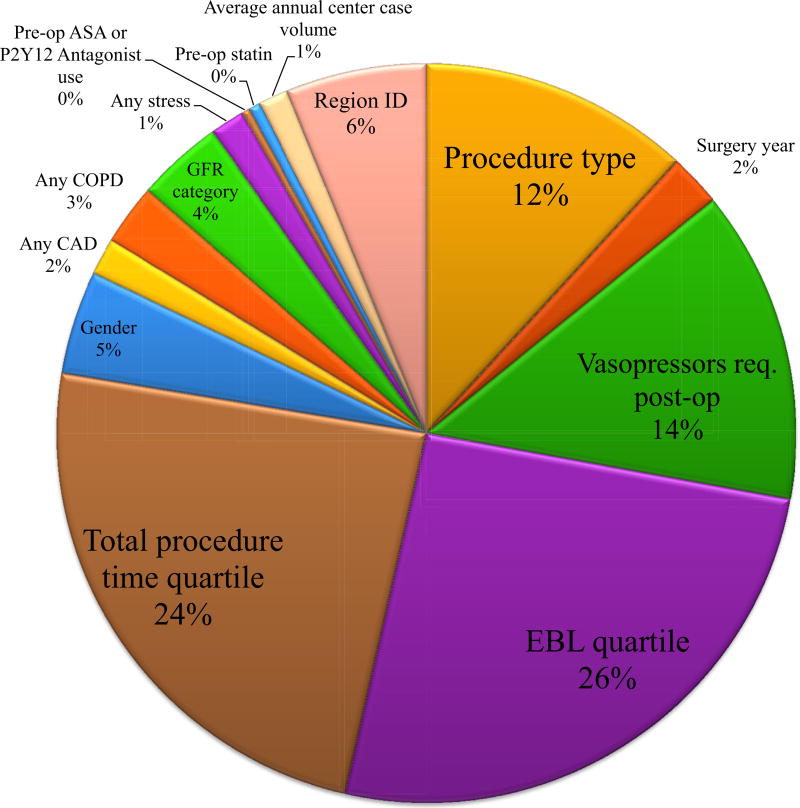
Results: The 7171 patients undergoing abdominal aortic surgery were a mean age of 65.4 (standard deviation, 10.2) years, and 63% were male. Extubation occurred (1) in the operating room (76.3%), (2) <12 hours (10.9%), (3) 12 to 24 hours (7.2%), or (4) >24 hours (5.6%) after surgery. Hospitals in the top quartile for case volume had the highest percentage of patients extubated in the operating room (82.8%). Patients least likely to be extubated in the operating room were older, more likely to have chronic obstructive pulmonary disease, require vasopressors, have higher estimated blood loss (EBL), and longer procedure times. After adjustment for patient, procedure, and institutional factors, delayed extubation was associated with prolonged LOS (<12 hours: odds ratio [OR], 1.4; 95% confidence interval [CI], 1.2-1.7; 12-24 hours: OR, 2.1; 95% CI, 1.7-2.7; >24 hours: OR, 5.3; 95% CI, 4.0-6.9), and pulmonary complications (<12 hours: OR, 1.9; 95% CI, 1.4-2.6; 12-24 hours: OR, 2.6; 95% CI, 1.8-3.6; >24 hours: OR, 9.6; 95% CI, 7.1-13.0) compared with those extubated in the operating room. Subset analysis of patients extubated in the operating room or <12 hours showed that extubation out of the operating room was associated with prolonged LOS (OR, 1.4; 95% CI, 1.2-1.7) and pulmonary complications (OR, 1.8; 95% CI, 1.3-2.5). The variable importance analysis demonstrated that EBL (26%) and procedure time (24%) accounted for half of the variation in extubation timing.
Conclusions: Extubation in the operating room is associated with shorter LOS and morbidity after open aortic surgery. EBL, procedure time, and center variation account for variability in extubation timing. These data advocate for standardized perioperative respiratory care to reduce variation, improve outcomes, and reduce LOS.
Copyright © 2017 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures

References
-
- EVAR trial participants. Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. Lancet. 2005;365:2179–86. - PubMed
-
- Burgers LT, Vahl AC, Severens JL, Wiersema AM, Cuypers PW, Verhagen HJ, et al. Cost-effectiveness of elective endovascular aneurysm repair versus open surgical repair of abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2016;52:29–40. - PubMed
-
- Dryjski M, O’Brien-Irr MS, Hassett J. Hospital costs for endovascular and open repair of abdominal aortic aneurysm. J Am Coll Surg. 2003;197:64–70. - PubMed
-
- Epstein D, Sculpher MJ, Powell JT, Thompson SG, Brown LC, Greenhalgh RM. Long-term cost-effectiveness analysis of endovascular versus open repair for abdominal aortic aneurysm based on four randomized clinical trials. Br J Surg. 2014;101:623–31. - PubMed
-
- Sternbergh WC, 3rd, Money SR. Hospital cost of endovascular versus open repair of abdominal aortic aneurysms: a multicenter study. J Vasc Surg. 2000;31:237–44. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
