

Comparison of Effort of Breathing for Infants on Nasal Modes of Respiratory Support
- PMID: 28366356
- PMCID: PMC5529226
- DOI: 10.1016/j.jpeds.2017.02.060
Comparison of Effort of Breathing for Infants on Nasal Modes of Respiratory Support
Abstract
Objective: To directly compare effort of breathing between high flow nasal cannula (HFNC), nasal intermittent mechanical ventilation (NIMV), and nasal continuous positive airway pressure (NCPAP).
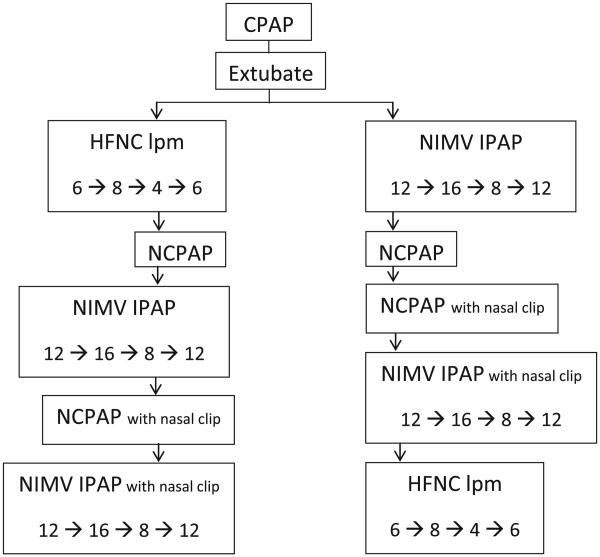
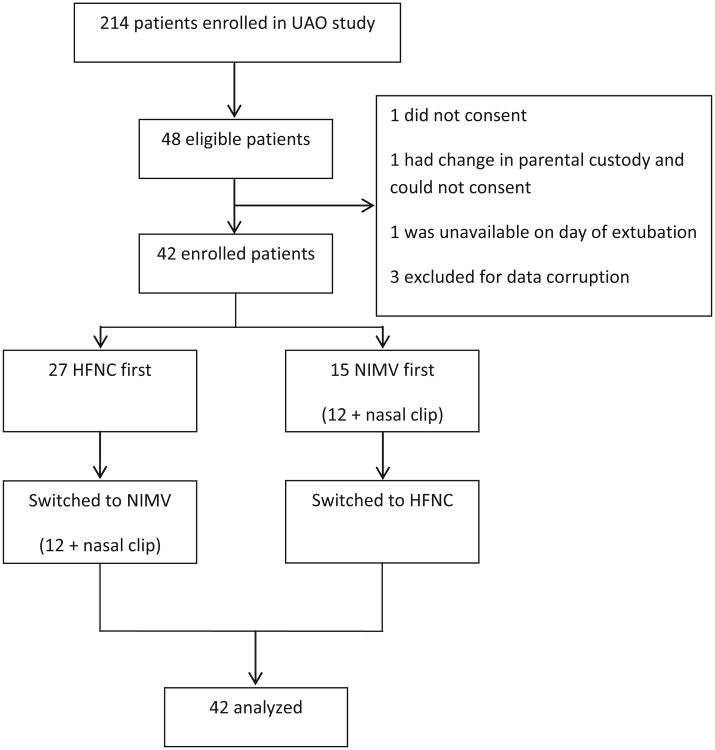
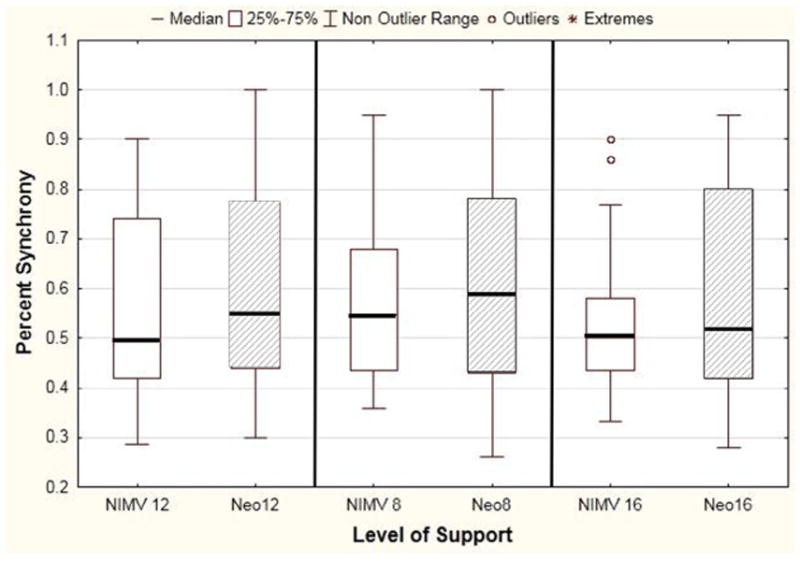
Study design: This was a single center prospective cross-over study for patients <6 months in the cardiothoracic or pediatric intensive care unit receiving nasal noninvasive respiratory support after extubation. We measured effort of breathing using esophageal manometry with pressure-rate product (PRP) on all 3 modes. NIMV synchrony was determined by comparing patient efforts (esophageal manometry) with mechanically delivered breaths (spirometry in ventilator circuit). On NIMV, PRP and synchrony was also measured after adding a nasal clip on 26 patients.
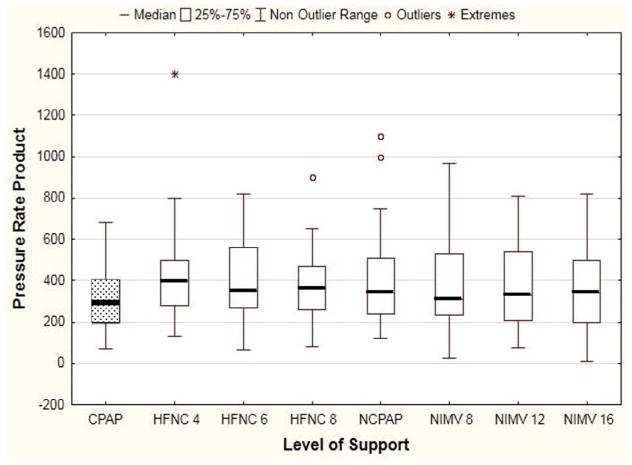
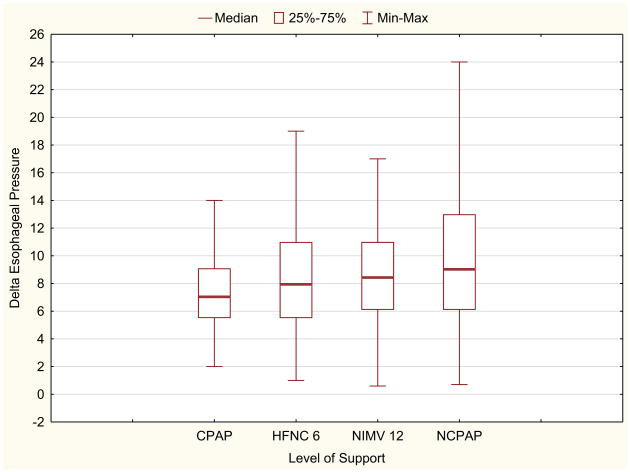
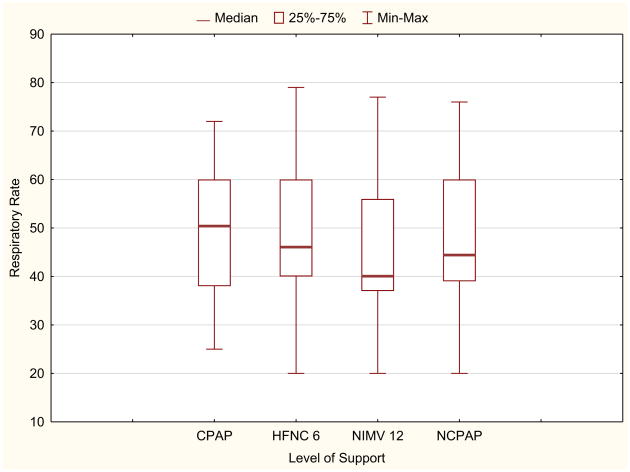
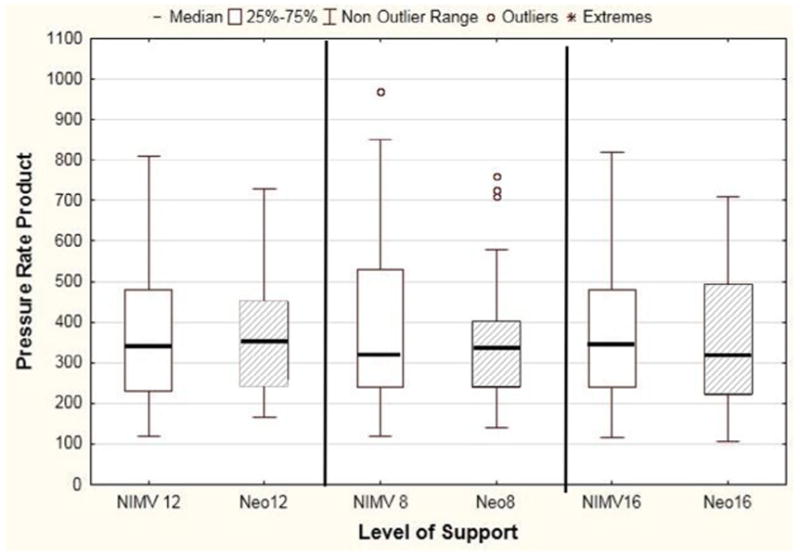
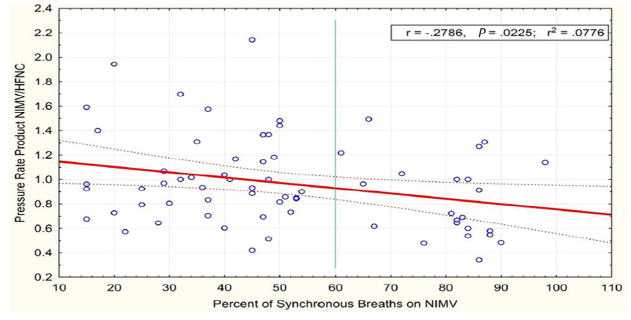
Results: Forty-two children were included. Median (IQR) age was 2 (0.5, 4) months. There was no difference in median PRP between HFNC 6 liters per minute, 355 (270,550), NIMV 12/5 cm H2O, 341 (235, 472), and NCPAP 5 cm H2O, 340 (245,506) (P?=?.33). Results were similar regardless of HFNC flow rate or NIMV inspiratory pressure. Median PRP on CPAP of 5 cm H2O prior to extubation 255 (176, 375) was significantly lower than all postextubation values (P?<?.002). On NIMV, less than 50% of patient efforts resulted in a ventilator breath, which was not improved with a nasal clip (P?>?.07)). However, as NIMV synchrony improved (>60%), PRP on NIMV was lower than on HFNC.
Conclusions: For infants, effort of breathing is similar on HFNC, NIMV, and NCPAP after extubation, regardless of flow rate or inspiratory pressure. We speculate that bi-level NIMV may be superior if high levels of synchrony can be achieved.
Keywords: humidified high flow nasal cannula; nasal continuous positive airway pressure; nasal intermittent mechanical ventilation.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Resistance of the interface device used to deliver nasal continuous positive airway pressure or nasal intermittent ventilation.J Pediatr. 2018 Feb;193:277. doi: 10.1016/j.jpeds.2017.10.045. Epub 2017 Dec 1. J Pediatr. 2018. PMID: 29198535 No abstract available.
-
Reply.J Pediatr. 2018 Feb;193:277. doi: 10.1016/j.jpeds.2017.10.061. J Pediatr. 2018. PMID: 29389449 No abstract available.
References
-
- Nava S. Behind a mask: tricks, pitfalls, and prejudices for noninvasive ventilation. Respir Care. 2013;58:1367–76. - PubMed
-
- Essouri S, Laurent M, Chevret L, Durand P, Ecochard E, Gajdos V, et al. Response to Jones et al.: revisiting the benefits of nCPAP versus intubation for severe bronchiolitis. Intensive Care Med. 2014;40:764. - PubMed
-
- Essouri S, Chevret L, Durand P, Haas V, Fauriux B, Devictor D. Noninvasive positive pressure ventilation: five years of experience in a pediatric intensive care unit. Pediatr Crit Care Med. 2006;7:329–34. - PubMed
-
- Essouri S, Durand P, Chevret L, Balu L, Devictor D, Fauroux B, et al. Optimal level of nasal continuous positive airway pressure in severe viral bronchiolitis. Intensive Care Med. 2011;37:2002–7. - PubMed
-
- Ganu S, Gautam A, Wilkins B, Egan J. Increase in use of noninvasive ventilation for infants with severe bronchiolitis is associated with decline in intubation rates over a decade. Intensive Care Med. 2012;38:1177–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
