

Prognostic Value of National Comprehensive Cancer Network Lung Cancer Resection Quality Criteria
- PMID: 28366464
- PMCID: PMC5401641
- DOI: 10.1016/j.athoracsur.2017.01.098
Prognostic Value of National Comprehensive Cancer Network Lung Cancer Resection Quality Criteria
Abstract
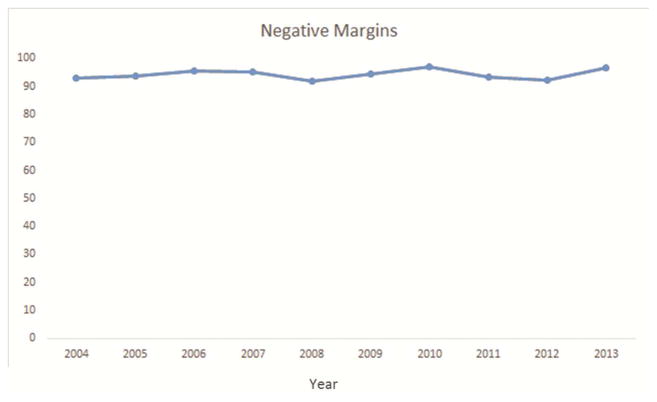
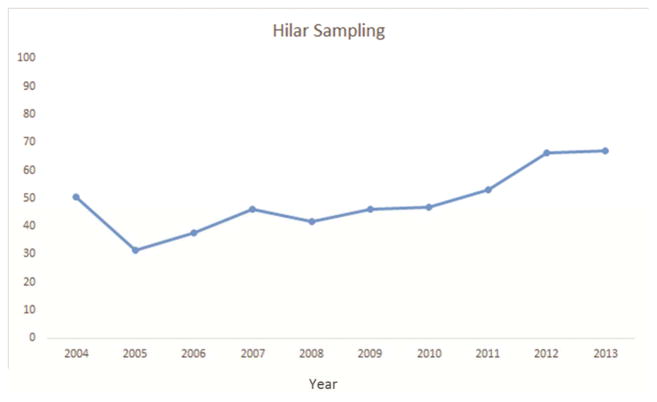
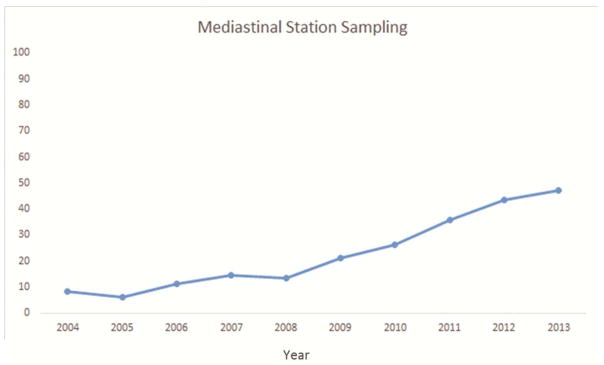
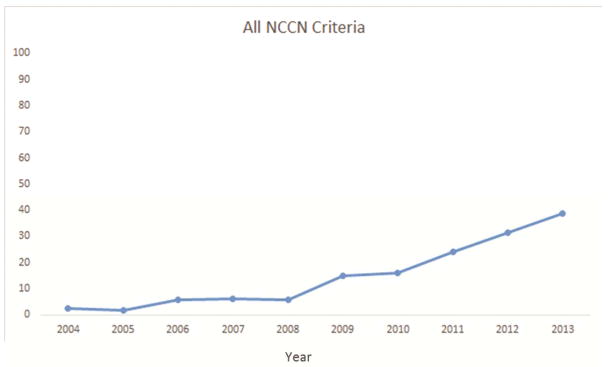
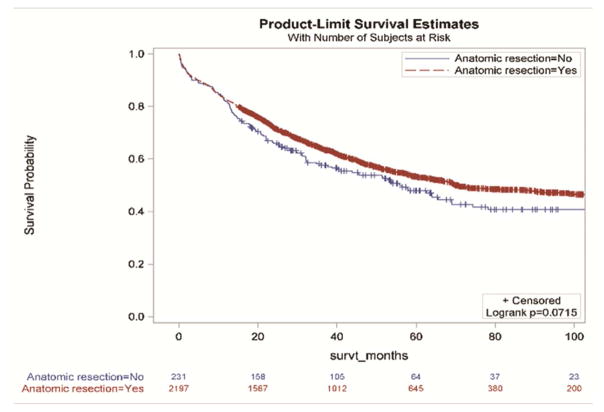
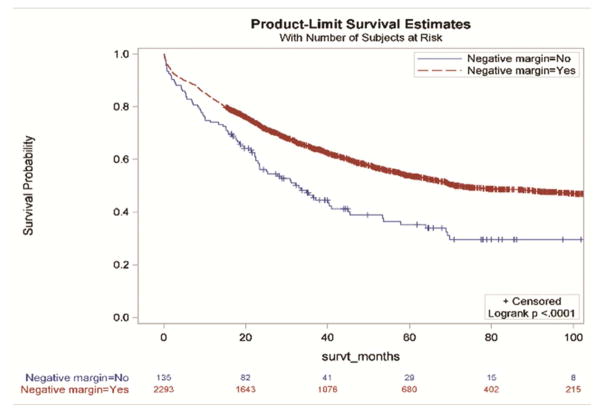
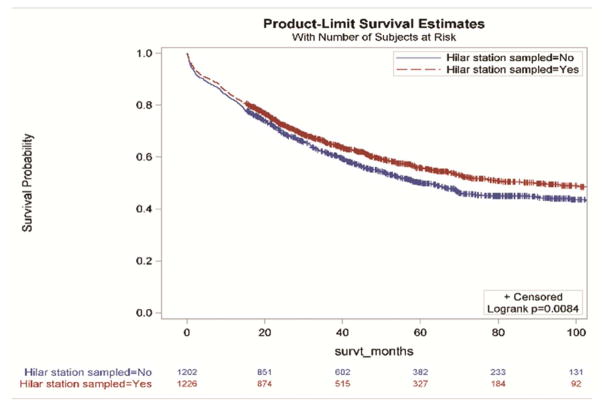
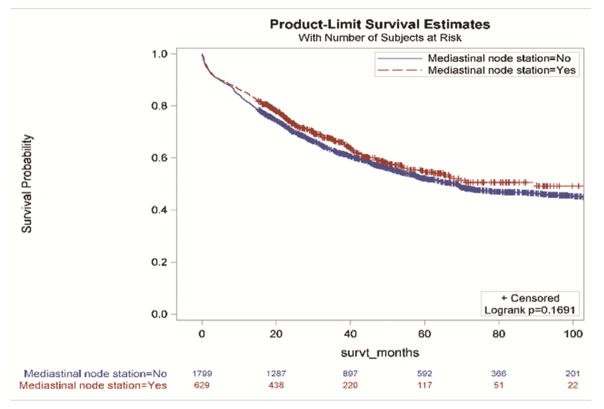
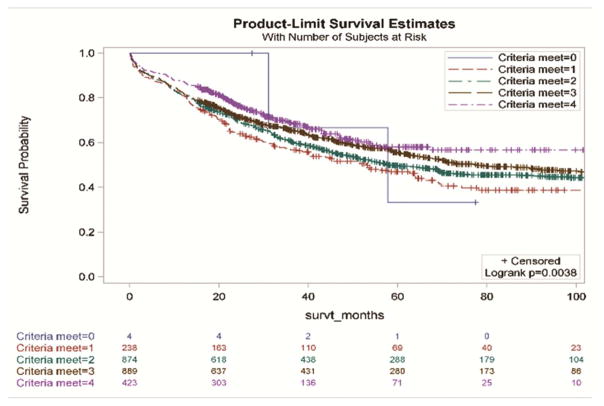
Background: The National Comprehensive Cancer Network (NCCN) surgical resection guidelines for non-small cell lung cancer recommend anatomic resection, negative margins, examination of hilar/intrapulmonary lymph nodes, and examination of three or more mediastinal nodal stations. We examined the survival impact of these criteria.
Methods: A population-based observational study was done using patient-level data from all curative-intent, non-small cell lung cancer resections from 2004 to 2013 at 11 institutions in four contiguous Dartmouth Hospital referral regions in three US states. We used an adjusted Cox proportional hazards model to assess the overall survival impact of attaining NCCN guidelines.
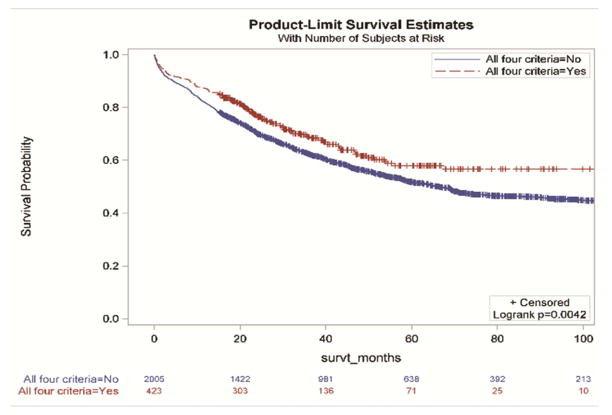
Results: Of 2,429 eligible resections, 91% were anatomic, 94% had negative margins, 51% sampled hilar nodes, and 26% examined three or more mediastinal nodal stations. Only 17% of resections met all four criteria; however, there was a significant increasing trend from 2% in 2004 to 39% in 2013 (p < 0.001). Compared with patients whose surgery missed one or more criteria, the hazard ratio for patients whose surgery met all four criteria was 0.71 (95% confidence interval: 0.59 to 0.86, p < 0.001). Margin status and the nodal staging criteria were most strongly linked with survival.
Conclusions: Attainment of NCCN surgical quality guidelines was low, but improving, over the past decade in this cohort from a high lung cancer mortality region of the United States. The NCCN quality criteria, especially the nodal examination criteria, were strongly associated with survival. The quality of nodal examination should be a focus of quality improvement in non-small cell lung cancer care.
Copyright © 2017 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Bach PB, Cramer LD, Schrag D, Downey RJ, Gelfand SE, Begg CB. The influence of hospital volume on survival after resection for lung cancer. N Engl J Med. 2001;345:181–8. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;846:1128–37. - PubMed
-
- Meguid RA, Brooke BS, Chang DC, Sherwood JT, Brock MV, Yang SC. Are surgical outcomes for lung cancer resections improved at teaching hopsitals? Ann Thorac Surg. 2008;85:1015–25. - PubMed
-
- Farjah F, Glum DR, Varghese TK, Symons RG, Wood DE. Surgeon specialty and long-term survival after pulmonary resection for lung cancer. Ann Thorac Surg. 2009;87:995–1006. - PubMed
-
- Schipper PH, Diggs BS, Ungerleider RM, Welke KF. The influence of surgeon specialty on outcomes in general thoracic surgery: a national sample 1996 to 2005. Ann Thorac Surg. 2009;88:1566–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
