

Intraoperative management of critical arrhythmia
- PMID: 28367281
- PMCID: PMC5370296
- DOI: 10.4097/kjae.2017.70.2.120
Intraoperative management of critical arrhythmia
Abstract
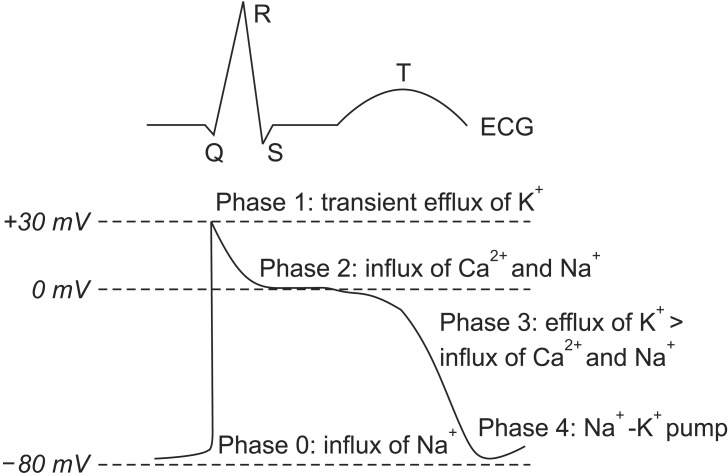
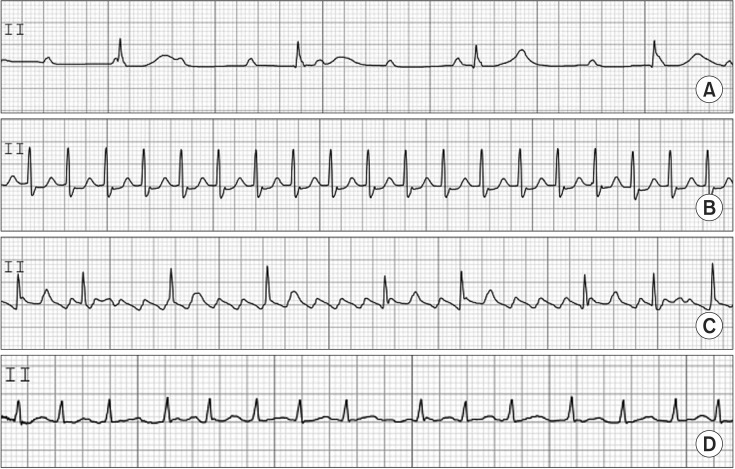
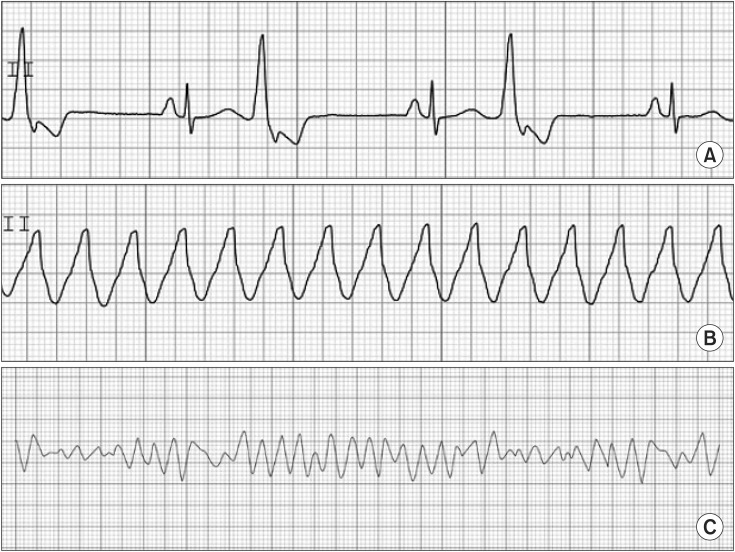
The incidence of intraoperative arrhythmia is extremely high, and some arrhythmias require clinical attention. Therefore, it is essential for the anesthesiologist to evaluate risk factors for arrhythmia and understand their etiology, electrophysiology, diagnosis, and treatment. Anesthetic agents reportedly affect normal cardiac electrical activity. In the normal cardiac cycle, the sinoatrial node initiates cardiac electrical activity through intrinsic autonomous pacemaker activity. Sequential atrial and ventricular contractions result in an effective cardiac pumping mechanism. Arrhythmia occurs due to various causes, and the cardiac pumping mechanism may be affected. A severe case may result in hemodynamic instability. In this situation, the anesthesiologist should eliminate the possible causes of arrhythmia and manage the condition, creating hemodynamic stability under proper electrocardiographic monitoring.
Keywords: Anesthesia; Cardiac arrhythmias; Cardiac cycle.
Figures


References
-
- Forrest JB, Cahalan MK, Rehder K, Goldsmith CH, Levy WJ, Strunin L, et al. Multicenter study of general anesthesia. II. Results. Anesthesiology. 1990;72:262–268. - PubMed
-
- Forrest JB, Rehder K, Cahalan MK, Goldsmith CH. Multicenter study of general anesthesia. III. Predictors of severe perioperative adverse outcomes. Anesthesiology. 1992;76:3–15. - PubMed
-
- Dua N, Kumra VP. Management of perioperative arrhythmias. Indian J Anaesth. 2007;51:310–323.
-
- Staikou C, Stamelos M, Stavroulakis E. Impact of anaesthetic drugs and adjuvants on ECG markers of torsadogenicity. Br J Anaesth. 2014;112:217–230. - PubMed
-
- Viskin S. Long QT syndromes and torsade de pointes. Lancet. 1999;354:1625–1633. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
