

Bypass surgery for chronic lower limb ischaemia
- PMID: 28368090
- PMCID: PMC6478298
- DOI: 10.1002/14651858.CD002000.pub3
Bypass surgery for chronic lower limb ischaemia
Abstract
Background: Bypass surgery is one of the mainstay treatments for patients with critical lower limb ischaemia (CLI). This is the second update of the review first published in 2000.
Objectives: To assess the effects of bypass surgery in patients with chronic lower limb ischaemia.
Search methods: For this update, the Cochrane Vascular Group searched its trials register (last searched October 2016) and the Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library (last searched Issue 9, 2016).
Selection criteria: We selected randomised controlled trials of bypass surgery versus control or any other treatment. The primary outcome parameters were defined as early postoperative non-thrombotic complications, procedural mortality, clinical improvement, amputation, primary patency, and mortality within follow-up.
Data collection and analysis: For the update, two review authors extracted data and assessed trial quality. We analysed data using odds ratio (OR) and 95% confidence intervals (CIs). We applied fixed-effect or random-effects models.
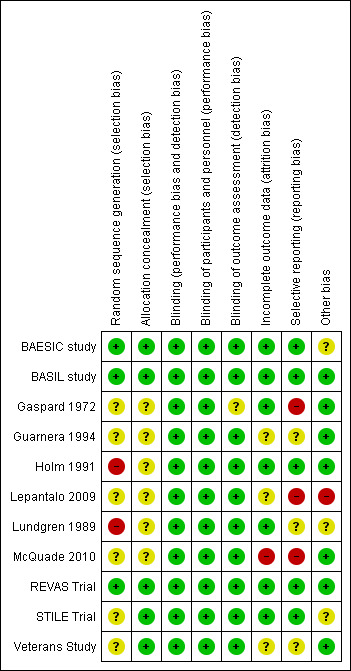
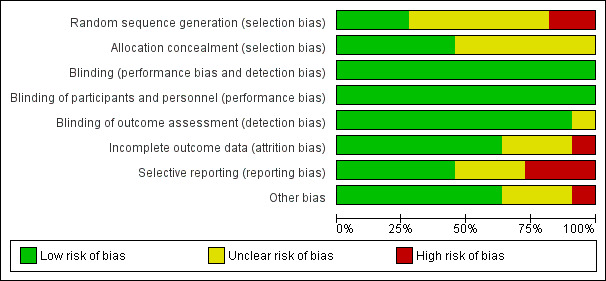
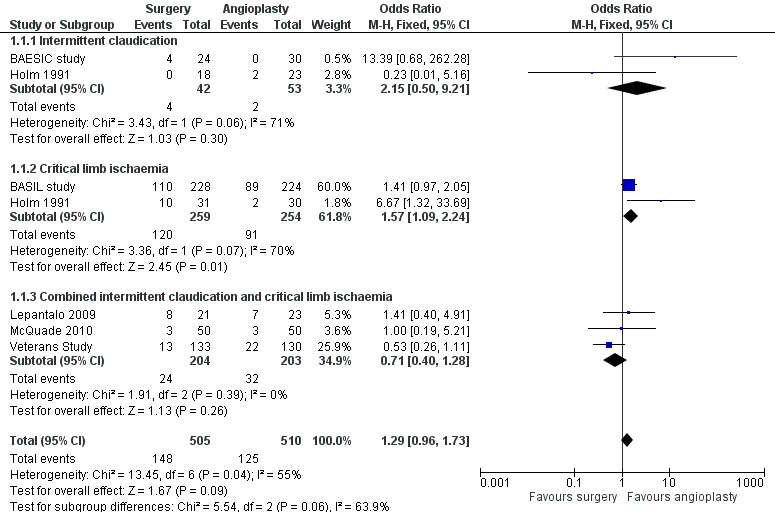
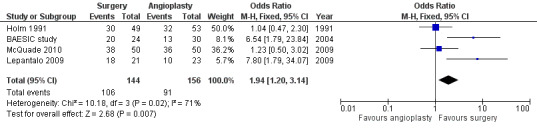
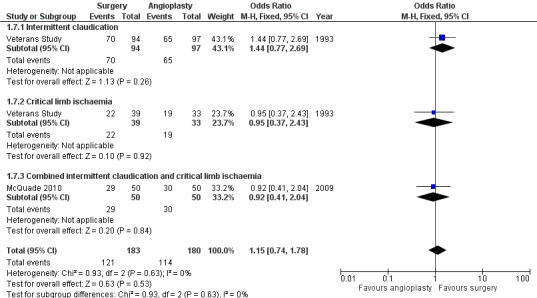
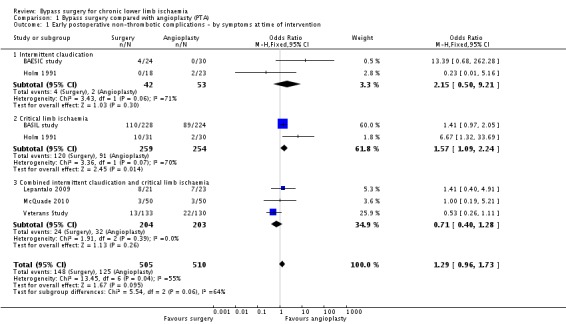
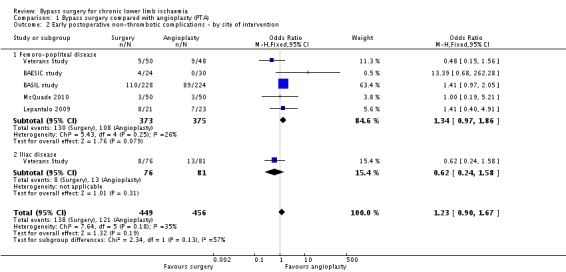
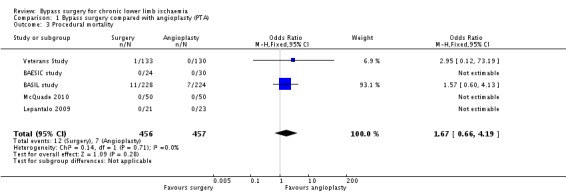
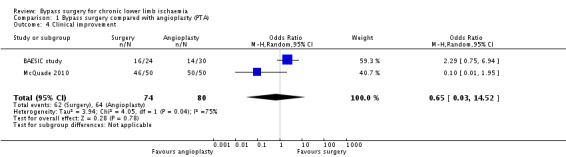
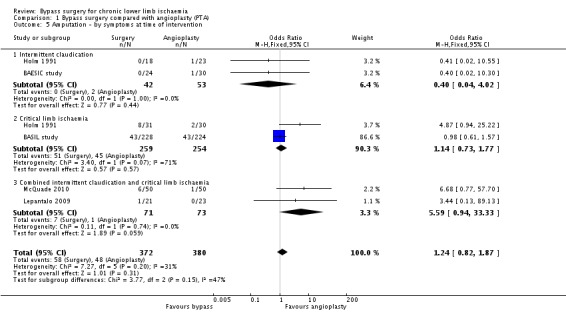
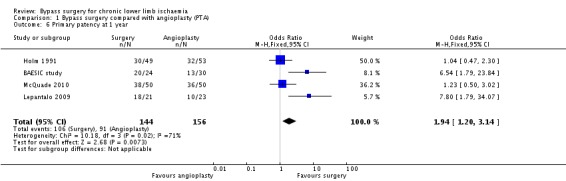
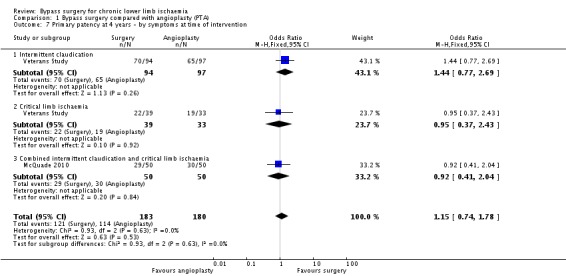
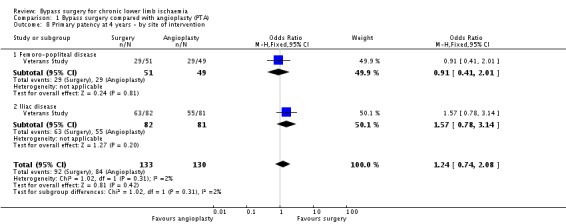
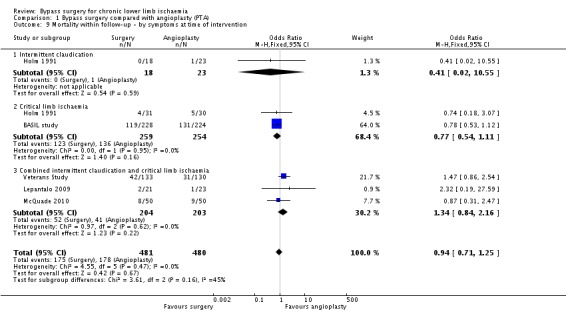
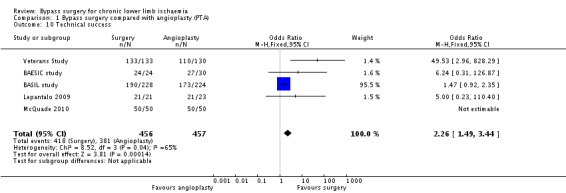
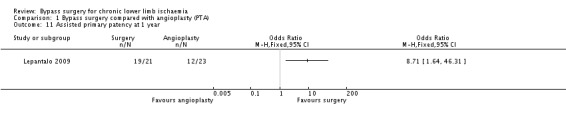
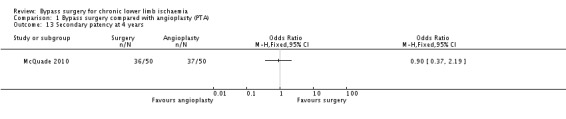
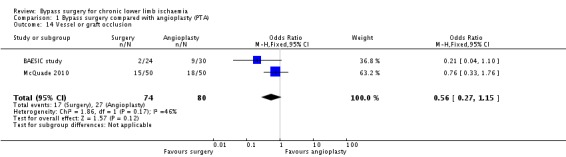
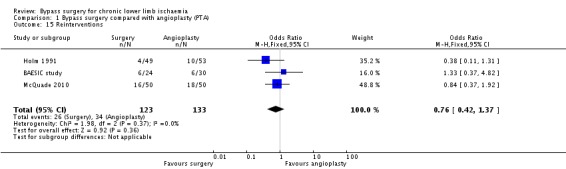
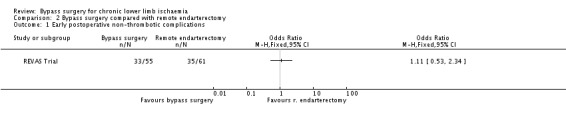
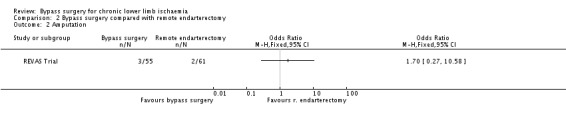
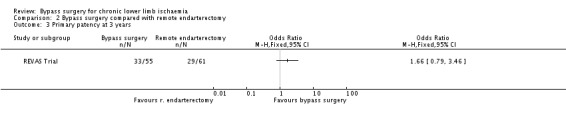
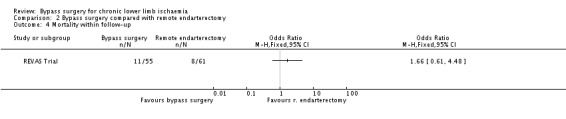
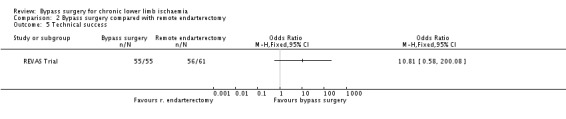
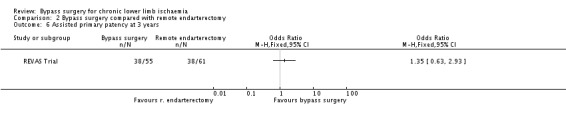
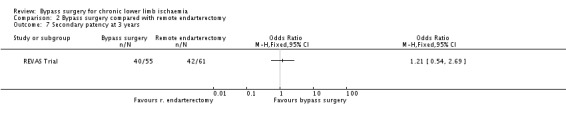
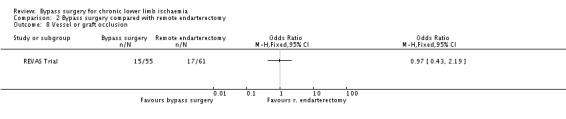
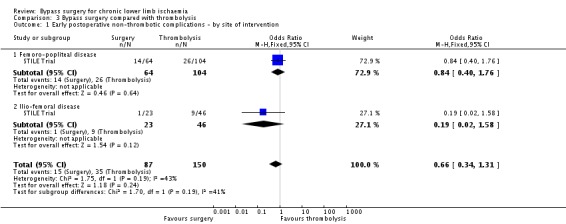
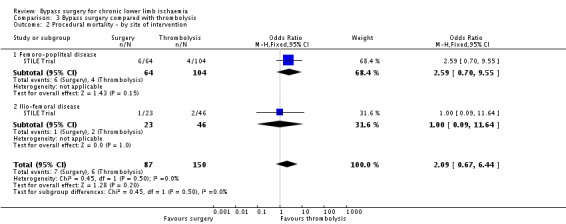
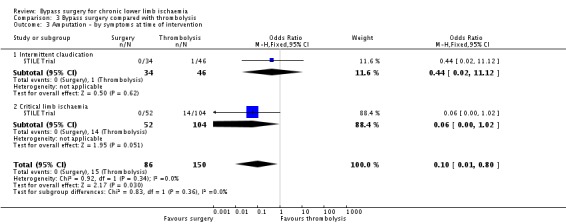
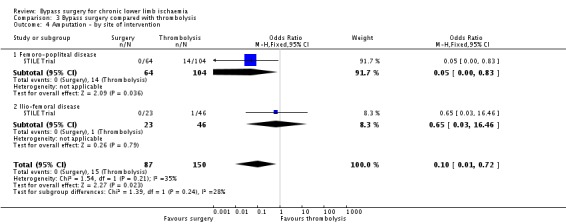
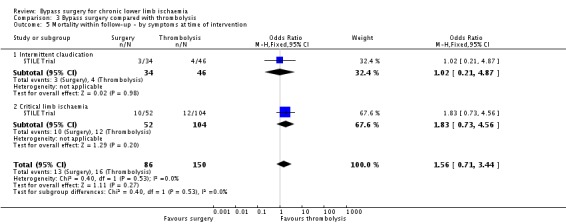
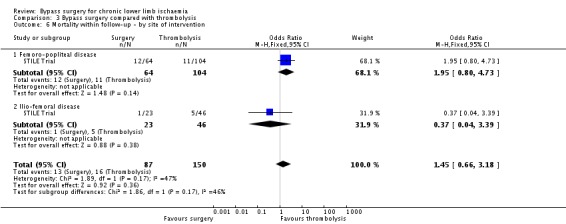
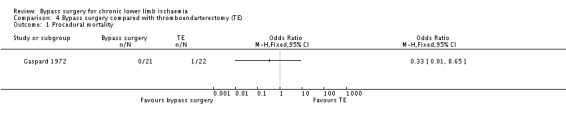
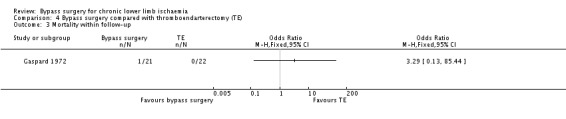
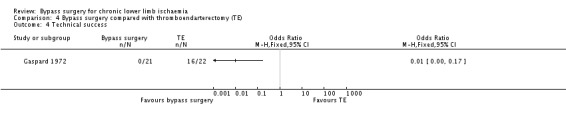
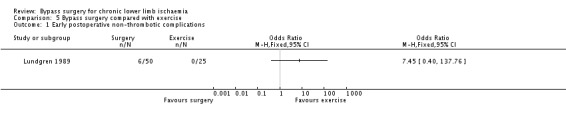
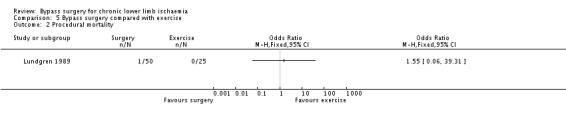
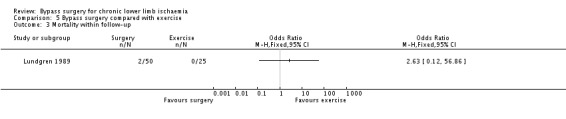
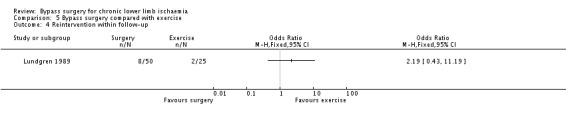
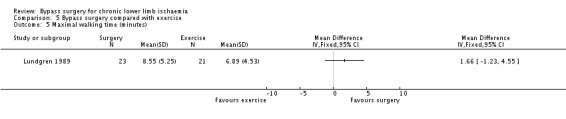
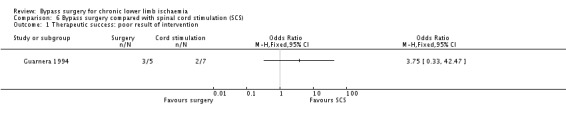
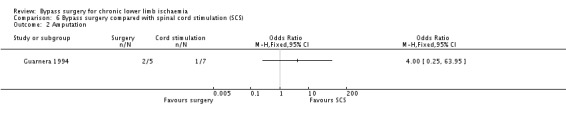
Main results: We selected 11 trials reporting a total of 1486 participants. Six trials compared bypass surgery with percutaneous transluminal angioplasty (PTA), and one each with remote endarterectomy, thromboendarterectomy, thrombolysis, exercise, and spinal cord stimulation. The quality of the evidence for the most important outcomes of bypass surgery versus PTA was high except for clinical improvement and primary patency. We judged the quality of evidence for clinical improvement to be low, due to heterogeneity between the studies and the fact that this was a subjective outcome assessment and, therefore, at risk of detection bias. We judged the quality of evidence for primary patency to be moderate due heterogeneity between the studies. For the remaining comparisons, the evidence was limited. For several outcomes, the CIs were wide.Comparing bypass surgery with PTA revealed a possible increase in early postinterventional non-thrombotic complications (OR 1.29, 95% CI 0.96 to 1.73; six studies; 1015 participants) with bypass surgery, but bypass surgery was associated with higher technical success rates (OR 2.26, 95% CI 1.49 to 3.44; five studies; 913 participants). Analyses by different clinical severity of disease (intermittent claudication (IC) or CLI) revealed that peri-interventional complications occurred more frequently in participants with CLI undergoing bypass surgery than PTA (OR 1.57, 95% CI 1.09 to 2.24). No differences in periprocedural mortality were identified (OR 1.67, 95% CI 0.66 to 4.19; five studies; 913 participants). The primary patency rate at one year was higher after bypass surgery than after PTA (OR 1.94, 95% CI 1.20 to 3.14; four studies; 300 participants), but this difference was not shown at four years (OR 1.15, 95% CI 0.74 to 1.78; two studies; 363 participants). No differences in clinical improvement (OR 0.65, 95% CI 0.03 to 14.52; two studies; 154 participants), amputation rates (OR 1.24, 95% CI 0.82 to 1.87; five studies; 752 participants), reintervention rates (OR 0.76, 95% CI 0.42 to 1.37; three studies; 256 participants), or mortality within the follow-up period (OR 0.94, 95% CI 0.71 to 1.25; five studies; 961 participants) between surgical and endovascular treatment were identified. No differences in subjective outcome parameters, indicated by quality of life and physical and psychosocial well-being, were reported. The hospital stay for the index procedure was reported to be longer in participants undergoing bypass surgery than in those treated with PTA.In the single study (116 participants) comparing bypass surgery with remote endarterectomy of the superficial femoral artery, the frequency of early postinterventional non-thrombotic complications was similar in the treatment groups (OR 1.11, 95% CI 0.53 to 2.34). No mortality within 30 days of the index treatment or during stay in hospital in either group was recorded. No differences were identified in patency (OR 1.66, 95% CI 0.79 to 3.46), amputation (OR 1.70, 95% CI 0.27 to 10.58), and mortality rates within the follow-up period (OR 1.66, 95% CI 0.61 to 4.48). Information regarding clinical improvement was unavailable.No differences in major complications (OR 0.66, 95% CI 0.34 to 1.31) or mortality (OR 2.09, 95% CI 0.67 to 6.44) within 30 days of treatment between surgery and thrombolysis (one study, 237 participants) for chronic lower limb ischaemia were identified. The amputation rate was lower after bypass surgery (OR 0.10, 95% CI 0.01 to 0.80). No differences in late mortality were found (OR 1.56, 95% CI 0.71 to 3.44). No data regarding patency rates and clinical improvement were reported.Technical success resulting in blood flow restoration was higher after bypass surgery than thromboendarterectomy for aorto-iliac occlusive disease (one study, 43 participants) (OR 0.01, 95% CI 0 to 0.17). The periprocedural mortality (OR 0.33, 95% CI 0.01 to 8.65), follow-up mortality (OR 3.29, 95% CI 0.13 to 85.44), and amputation rates (OR 0.47, 95% CI 0.08 to 2.91) did not differ between treatments. Clinical improvement and patency rates were not reported.Comparing surgery and exercise (one study, 75 participants) did not identify differences in early postinterventional complications (OR 7.45, 95% CI 0.40 to 137.76) and mortality (OR 1.55, 95% CI 0.06 to 39.31). The remaining primary outcomes were not reported. There was no difference in maximal walking time between exercise and surgery (1.66 min, 95% CI -1.23 to 4.55).Regarding comparisons of bypass surgery with spinal cord stimulation for CLI, there was no difference in amputation rates after 12 months of follow-up (OR 4.00, 95% CI 0.25 to 63.95; one study, 12 participants). The remaining primary outcome parameters were not reported.
Authors' conclusions: There is limited high quality evidence for the effectiveness of bypass surgery compared with other treatments; no studies compared bypass to optimal medical treatment. Our analysis has shown that PTA is associated with decreased peri-interventional complications in participants treated for CLI and shorter hospital stay compared with bypass surgery. Surgical treatment seems to confer improved patency rates up to one year. Endovascular treatment may be advisable in patients with significant comorbidity, rendering them high risk surgical candidates. No solid conclusions can be drawn regarding comparisons of bypass surgery with other treatments because of the paucity of available evidence. Further large trials evaluating the impact of anatomical location and extent of disease and clinical severity are required.
Conflict of interest statement
GAA: none known GSG: none known SAA: received travel and accommodation expenses relating to the duties of the Journal and Publication Committee Members of the European Association for Endoscopic Surgery (EAES); travel, accommodation and congress participation expenses for the 21st International Congress of the EAES; travel and accommodation expenses for presentation of part of the Guidelines on the Closure of Abdominal Wall Incisions at the 36th International Congress of the European Hernia Society; travel and accommodation expenses for the development of the Guidelines on the Closure of Abdominal Wall Incisions RRM: none known JDS: received educational sponsorship (accommodation and course fee) from Cook Ltd for attendance at 2015 Leipzig Interventional Course (GORE Ltd). No personal payments were made. FT: received educational sponsorship (travel, accommodation and meeting‐related expenses) from Endologix Inc. This company produces medical devices. Such devices are not used for treatment of peripheral arterial disease and do not bear any direct relevance to the topic of this review.
Figures



Update of
-
Bypass surgery for chronic lower limb ischaemia.Cochrane Database Syst Rev. 2008 Apr 16;(2):CD002000. doi: 10.1002/14651858.CD002000.pub2. Cochrane Database Syst Rev. 2008. Update in: Cochrane Database Syst Rev. 2017 Apr 03;4:CD002000. doi: 10.1002/14651858.CD002000.pub3. PMID: 18425879 Updated.
References
References to studies included in this review
BAESIC study {published data only}
-
- Zaag ES, Legemate DA, Prins MH, Reekers JA, Jacobs MJ. Angioplasty or bypass for superficial femoral artery disease? A randomised controlled trial. European Journal of Vascular and Endovascular Surgery 2004;28(2):132‐7. - PubMed
BASIL study {published data only}
-
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, et al. BASIL trial participants. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet 2005;366(9501):1925‐34. - PubMed
-
- Bell J, Papp L, Bradbury AW. Bypass or angioplasty for severe ischaemia of the leg: the BASIL trial. In: Greenhalgh RM, Powell JT, Mitchell AW editor(s). Vascular and endovascular opportunities. London: WB Saunders, 2000:485‐94.
-
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, Gillespie I, et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: A description of the severity and extent of disease using the Bollinger angiogram scoring method and the TransAtlantic Inter‐Society Consensus II classification. Journal of Vascular Surgery 2010;51(5 Supplement 1):32S‐42S. - PubMed
-
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, Gillespie I, et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: A survival prediction model to facilitate clinical decision making. Journal of Vascular Surgery 2010;51(5 Suppl 1):52S‐68S. - PubMed
-
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, Gillespie I, et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: An intention‐to‐treat analysis of amputation‐free and overall survival in patients randomized to a bypass surgery‐first or a balloon angioplasty‐first revascularization strategy. Journal of Vascular Surgery 2010;51(5 Supplement 1):5S‐17S. - PubMed
Gaspard 1972 {published data only}
-
- Gaspard DJ, Cohen JL, Gaspar MR. Aortoiliofemoral thromboendarterectomy vs bypass graft. Archives of Surgery 1972;105(6):898‐901. - PubMed
Guarnera 1994 {published data only}
-
- Guarnera G, Furgiuele S, Camilli S. Spinal cord electric stimulation vs femoro‐distal bypass in critical ischaemia of the legs. Preliminary results of a prospective randomised study [Elettrostimolazione midollare vs bypass femoro‐distale nell'ischemia critica arti inferiori. Risultati preliminari di uno prospettico randomizzato]. Minerva Cardioangiologica 1994;42(5):223‐7. - PubMed
Holm 1991 {published data only}
-
- Holm J, Arfvidsson B, Jivegard L, Lundgren F, Lundholm K, Schersten T, et al. Chronic lower limb ischaemia. A prospective randomised controlled study comparing the 1‐year results of vascular surgery and percutaneous transluminal angioplasty (PTA). European Journal of Vascular Surgery 1991;5(5):517‐22. - PubMed
Lepantalo 2009 {published data only}
-
- Lepäntalo M, Laurila K, Roth WD, Rossi P, Lavonen J, Mäkinen K, et al. PTFE bypass or thrupass for superficial femoral artery occlusion? A randomised controlled trial. European Society for Vascular Surgery Annual Meeting; 2008 Sep 4‐7, Nice, France. 2008. - PubMed
-
- Lepäntalo M, Laurila K, Roth WD, Rossi P, Lavonen J, Mäkinen K, et al. Scandinavian Thrupass Study Group. PTFE bypass or thrupass for superficial femoral artery occlusion? A randomised controlled trial. European Journal of Vascular and Endovascular Surgery 2009;37:578‐84. - PubMed
Lundgren 1989 {published data only}
-
- Lundgren F, Dahllof AG, Schersten T, Bylund‐Fellenius AC. Muscle enzyme adaptation in patients with peripheral arterial insufficiency: spontaneous adaptation, effect of different treatments and consequences on walking performance. Clinical Science 1989;77(5):485‐93. - PubMed
McQuade 2010 {published data only}
-
- Kedora J, Hohmann S, Garrett W, Munschaur C, Theune B, Gable D. Randomized comparison of percutaneous Viabahn stent grafts vs prosthetic femoral‐popliteal bypass in the treatment of superficial femoral arterial occlusive disease. Journal of Vascular Surgery 2007;45:10‐16. - PubMed
-
- McQuade K, Gable D, Hohman S, Pearl G, Theune B. Randomized comparison of ePTFE/nitinol self‐expanding stent graft vs prosthetic femoral‐popliteal bypass in the treatment of superficial femoral artery occlusive disease. Journal of Vascular Surgery 2009;49:109‐16. - PubMed
-
- McQuade K, Gable D, Pearl G, Theune B, Black S. Four‐year randomized prospective comparison of percutaneous ePTFE/nitinol self‐expanding stent graft versus prosthetic femoral‐popliteal bypass in the treatment of superficial femoral artery occlusive disease. Journal of Vascular Surgery 2010;52:584‐91. - PubMed
REVAS Trial {published data only}
-
- Gisbertz SS, Ramzan M, Tutein Nolthenius RP, Laan L, Overtoom TT, Moll FL, et al. Short‐term results of a randomized trial comparing remote endarterectomy and supragenicular bypass surgery for long occlusions of the superficial femoral artery (the REVAS Trial). European Journal of Vascular and Endovascular Surgery 2009;37(1):68‐76. - PubMed
-
- Gisbertz SS, Tutein Nolthenius RP, Borst GJ, Laan L, Overtoom TT, Moll FL, et al. Remote endarterectomy versus supragenicular bypass surgery for long occlusions of the superficial femoral artery: medium‐term results of a randomized controlled trial (the REVAS trial). Annals of Vascular Surgery 2010;24(8):1015‐23. - PubMed
STILE Trial {published data only}
-
- Weaver FA, Comerota AJ, Youngblood M, Froehlich J, Hosking JD, Papanicolaou G, STILE Investigators. Surgical revascularization versus thrombolysis for nonembolic lower extremity native artery occlusions: results of a prospective randomized trial. The STILE Investigators. Surgery versus Thrombolysis for Ischemia of the Lower Extremity. Journal of Vascular Surgery 1996;24(4):513‐23. - PubMed
Veterans Study {published data only}
-
- Bergan JJ, Wilson SE, Wolf G, Deupree RH. Unexpected, late cardiovascular effects of surgery for peripheral artery disease. Archives of Surgery 1992;127(9):1119‐23, discussion 1123‐4. - PubMed
-
- Wilson SE, Wolf GL, Cross AP. Percutaneous transluminal angioplasty versus operation for peripheral arteriosclerosis. Journal of Vascular Surgery 1989;9(1):1‐9. - PubMed
-
- Wolf GL, Wilson SE, Cross AP, Deupree RH, Stason WB. Surgery or balloon angioplasty for peripheral vascular disease: a randomised clinical trial. Journal of Vascular and Interventional Radiology 1993;4(5):639‐48. - PubMed
References to studies excluded from this review
ABC 2010 {published data only}
-
- NCT01177033. Angioplasty or Bypass surgery in intermittent Claudication (ABC Trial). http://clinicaltrials.gov/show/NCT01177033 (accessed 24 September 2014).
CLEVER study {published data only}
-
- Murphy TPC, Massaro MR, Jaff S, Collins ME. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: Six‐month outcomes from the Claudication: Exercise Versus Endoluminal Revascularization (CLEVER) study. Circulation 2012;125(1):130‐9. - PMC - PubMed
de Donato 2002 {published data only}
-
- Donato G, Weber G, Donato G. Minimally invasive or conventional aorto‐bifemoral by‐pass. A randomised study. European Journal of Vascular and Endovascular Surgery 2002;24(6):485‐91. - PubMed
Devine 2004 {published data only}
-
- Devine C, McCollum C, North West Femoro‐Popliteal Trial Participants. Heparin‐bonded Dacron or polytetrafluorethylene for femoropopliteal bypass: five‐year results of a prospective randomized multicenter clinical trial. Journal of Vascular Surgery 2004;40(5):924‐31. - PubMed
Djoric 2011 {published data only}
-
- Djoric P. Early individual experience with distal venous arterialization as a lower limb salvage procedure. American Surgeon 2011;77(6):726‐30. - PubMed
Gavrilenko 2008 {published data only}
-
- Gavrilenko AV, Voronov DA, Konstantinov BA, Bochkov NP. Combination of reconstructive vascular operations with gene‐engineering technologies of angiogenesis stimulation: a present‐day policy aimed at improving the remote results of treating patients with lower limb chronic ischaemia. [Russian]. Angiologiia i Sosudistaia Khirurgiia/Angiology & Vascular Surgery 2008;14(4):49‐53. - PubMed
Gelin 2001 {published data only}
-
- Gelin J, Jivegard L, Taft C, Karlsson J, Sullivan M, Dahllöf AG, et al. Treatment efficacy of intermittent claudication by surgical intervention, supervised physical exercise training compared to no treatment in unselected randomised patients I: one year results of functional and physiological improvements. European Journal of Vascular and Endovascular Surgery 2001;22(2):107‐13. - PubMed
Hamsho 1999 {published data only}
-
- Hamsho A, Nott D, Harris PL. Prospective randomised trial of distal arteriovenous fistula as an adjunct to femoro‐infrapopliteal PTFE bypass. European Journal of Vascular and Endovascular Surgery 1999;17(3):197‐201. - PubMed
IRONIC Trial {published data only}
-
- NCT01219842. Invasive revascularization or not in intermittent claudication ‐ a randomised controlled trial IRONIC. http://clinicaltrials.gov/show/NCT01219842 (accessed 24 September 2014).
Jensen 2007 {published data only}
-
- Jensen LP, Lepantalo M, Fossdal JE, Roder OC, Jensen BS, Madsen MS, et al. Dacron or PTFE for above‐knee femoropopliteal bypass. A multicenter randomised study. European Journal of Vascular and Endovascular Surgery 2007;34(1):44‐9. - PubMed
Linhart 1991 {published data only}
-
- Linhart J, Vanek I. Treatment of intermittent claudication: two different mechanisms. International Angiology 1991;10(1):6‐9. - PubMed
Matyas 2008 {published data only}
-
- Mátyás L, Berry M, Menyhei G, Tamás L, Acsády G, Cuypers P, et al. The safety and efficacy of a paclitaxel‐eluting wrap for preventing peripheral bypass graft stenosis: a 2‐year controlled randomized prospective clinical study. European Journal of Vascular and Endovascular Surgery 2008;35:715‐22. - PubMed
McCollum 2003 {published data only}
-
- McCollum CN, Devine CM, the North West Femoro‐Popliteal Trial Participants. Heparin bonded dacron or polytetrafluoroethylene for femoro‐popliteal bypass: Five year results of a prospective randomised multi‐centre clinical trial. The Vascular Surgical Society of Great Britain and Ireland Yearbook 2003. 2003:67.
Mohammadi 2007 {published data only}
-
- Mohammadi TA, Warnier de WG, Rhissassi B. Comparing vein with collagen impregnated woven polyester prosthesis in above‐knee femoropopliteal bypass grafting. International Journal of Surgery 2007;5(2):109‐13. - PubMed
Nordanstig 2011 {published and unpublished data}
-
- Nordanstig J, Gelin J, Hensater M, Taft C, Osterberg K, Jivegard L. Walking performance and health‐related quality of life after surgical or endovascular invasive versus non‐invasive treatment for intermittent claudication ‐ a prospective randomised trial. European Journal of Vascular and Endovascular Surgery 2011;42(2):220‐7. - PubMed
Panneton 2004 {published data only}
-
- Panneton JM, Hollier LH, Hofer JM. Multicenter randomized prospective trial comparing a pre‐cuffed polytetrafluoroethylene graft to a vein cuffed polytetrafluoroethylene graft for infragenicular arterial bypass. Annals of Vascular Surgery 2004;18(2):199‐206. - PubMed
PROOF 2007 {published data only}
-
- NCT00504088. Plaque removal versus open bypass surgery for critical limb ischemia (PROOF). http://clinicaltrials.gov/show/NCT00504088 (accessed 24 September 2014).
Stanisic 2009 {published data only}
-
- Stanisic M, Bucko W, Majewski W. Hand‐assisted laparoscopic aortic surgery as an initial step toward totally laparoscopic techniques in patients with aorto‐iliac occlusion in critical limb ischaemia. Wideochirurgia I Inne Techniki Maloinwazyjne 2009;4:67‐71.
Taft 2004 {published data only}
-
- Taft C, Sullivan M, Lundholm K, Karlsson J, Gelin J, Jivegard L. Predictors of treatment outcome in intermittent claudication. European Journal of Vascular and Endovascular Surgery 2004;27(1):24‐32. - PubMed
TECCO Trial {published data only}
-
- Gouëffic Y. The TECCO trial: results of the French multicentric randomized clinical trial comparing endovascular vs open surgery for the treatment of common femoral artery de novo lesions. Leipzig Interventional Course 2014. 2014.
Tiek 2009 {published data only}
-
- Tiek J, Fourneau I, Daenens K, Nevelsteen A. The role of thrombolysis in acute infrainguinal bypass occlusion: a prospective nonrandomized controlled study. Annals of Vascular Surgery 2009;23:179‐85. - PubMed
Tiek 2012 {published data only}
-
- Tiek J, Remy P, Sabbe T, D'hont C, Houthoofd S, Daenens K, et al. Laparoscopic versus open approach for aortobifemoral bypass for severe aorto‐iliac occlusive disease ‐ a multicentre randomised controlled trial. European Journal of Vascular and Endovascular Surgery 2012;43(6):711‐5. - PubMed
Vukobratov 2006 {published data only}
-
- Vukobratov V, Kaanski M, Pasternak J, Nikoli D, Popovi V, Obradovi J, et al. Femoro‐popliteal reconstructions: "in situ" versus "reversed" technique: comparative results. Medicinski Pregled 2006;59(7‐8):360‐4. - PubMed
References to ongoing studies
BASIL 2 {published data only}
-
- Bradbury A. BASIL 2 randomised trial launched to address need for data for endovascular interventions for severe limb ischaemia. Charing Cross Symposium. 2014.
-
- ISRCTN27728689. BASIL 2 randomised trial launched to address need for data for endovascular interventions for severe limb ischaemia. ISRCTN Register 2014.
BEST‐CLI trial {published data only}
-
- Farber A, Rosenfield K, Menard M. The BEST‐CLI trial: A multidisciplinary effort to assess which therapy is best for patients with critical limb ischemia. Techniques in Vascular and Interventional Radiology 2014;17(3):221‐4. - PubMed
FINNPTX {published data only}
-
- NCT01450722. Paclitaxel eluting stent in long SFA obstruction: a prospective, randomized comparison with bypass surgery (finnptx). https://clinicaltrials.gov/ct2/show/NCT01450722 (accessed October 2016).
ISRCTN18315574 {published data only}
-
- ISRCTN18315574. Minimal invasive balloon expansion versus bypass operation to treat complicated occlusions and stenoses of the femoral and popliteal arteries. www.isrctn.com/ISRCTN18315574 (accessed October 2016).
NCT01171703 {published data only}
-
- NCT01171703. Optimized strategy for diabetic patients with critical limb ischemia (Part I) (DCLI‐I). clinicaltrials.gov/ct2/show/NCT01171703 (accessed October 2016).
NCT02580084 {published data only}
-
- NCT02580084. Clinical study of the aorta‐femoral bypass and hybrid intervention and the iliac arteries with stenting and plasty of the common femoral artery effectiveness in patients with the iliac segment and femoral artery occlusive disease (TASC C, D). clinicaltrials.gov/ct2/show/NCT02580084 (accessed October 2016).
ROBUST {published data only}
-
- Malas MBQ, Freischlag BA. Design of the revascularization with open bypass vs angioplasty and stenting of the lower extremity trial (ROBUST): a randomized clinical trial. JAMA Surgery 2014;149(12):1289‐95. [NCT01602159] - PubMed
-
- NCT01602159. Revascularization with Open Bypass versUs angioplasty and STenting of the lower extremity Trial (ROBUST). https://clinicaltrials.gov/ct2/show/NCT01602159 (accessed October 2016). - PubMed
SUPERB {published data only}
ZILVERPASS {published data only}
-
- NCT01952457. The Cook Zilver PTX drug‐eluting stent versus bypass surgery for the treatment the Cook Zilver PTX drug‐eluting stent versus bypass surgery of femoropopliteal TASC C&D Lesions (ZILVERPASS). http://clinicaltrials.gov/ct2/show/NCT01952457?term=NCT01952457&rank=1 (accessed October 2016).
Additional references
Abu Dabrh 2016
-
- Abu Dabrh AM, Steffen MW, Asi N, Undavalli C, Wang Z, Elamin MB, et al. Bypass surgery versus endovascular interventions in severe or critical limb ischemia. Journal of Vascular Surgery 2016; Vol. 63:244‐253e11. - PubMed
Acin 2012
-
- Acin F, Haro J, Bleda S, Varela C, Esparza L. Primary nitinol stenting in femoropopliteal occlusive disease: a meta‐analysis of randomized controlled trials. Journal of Endovascular Therapy 2012;19:585‐95. - PubMed
Antoniou 2008
-
- Antoniou GA, Koutsias S, Antoniou SA, Giannoukas AD. Remote endarterectomy for long segment superficial femoral artery occlusive disease. A systematic review. European Journal of Vascular and Endovascular Surgery 2008;36:310‐8. - PubMed
Antoniou 2009
-
- Antoniou GA, Sfyroeras GS, Karathanos C, Achouhan H, Koutsias S, Vretzakis G, et al. Hybrid endovascular and open treatment of severe multilevel lower extremity arterial disease. European Journal of Vascular and Endovascular Surgery 2009;38:616‐22. - PubMed
Antoniou 2013a
-
- Antoniou GA, Mavroforou A, Antoniou SA, Murray D, Kuhan G, Giannoukas AD. Evidence‐based medicine in vascular and endovascular practice. Journal of Endovascular Therapy 2013;20:678‐83. - PubMed
Antoniou 2013b
-
- Antoniou GA, Chalmers N, Georgiadis GS, Lazarides MK, Antoniou SA, Serracino‐Inglott F, et al. A meta‐analysis of endovascular versus surgical reconstruction of femoropopliteal arterial disease. Journal of Vascular Surgery 2013;57:242‐53. - PubMed
Antoniou 2014
-
- Antoniou GA, Georgakarakos EI, Antoniou SA, Georgiadis GS. Does endovascular treatment of infra‐inguinal arterial disease with drug‐eluting stents offer better results than angioplasty with or without bare metal stents?. Interactive Cardiovascular and Thoracic Surgery 2014;19:282‐5. - PubMed
Berridge 2013
Bradbury 2004
-
- Bradbury A, Wilmink T, Lee AJ, Bell J, Prescott R, Gillespie I, et al. Bypass versus angioplasty to treat severe limb ischemia: factors that affect treatment preferences of UK surgeons and interventional radiologists. Journal of Vascular Surgery 2004;39:1026‐32. - PubMed
Chang 2013
Fontaine 1954
-
- Fontaine R, Kim M, Kieny R. Surgical treatment of peripheral circulation disease [Die chirurgische Behandlung der peripheren Durchblutungsstorungen]. Helvetica Chirurgica Acta 1954;21(5‐6):499‐533. - PubMed
Fu 2015
GRADE 2004
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Holden 1950
-
- Holden WD. Reconstruction of the femoral artery for arteriosclerotic thrombosis. Surgery 1950;27:417.
Norgren 2007
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group. Inter‐society consensus for the management of peripheral arterial disease (TASC II). Journal of Vascular Surgery 2007;45 Suppl S:S5‐67. - PubMed
Rutherford 1997
-
- Rutherford RB, Baker JD, Ernst C, Johnston KW, Porter JM, Ahn S, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. Journal of Vascular Surgery 1997;26:517‐38. - PubMed
Selvin 2004
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999‐2000. Circulation 2004;110:738‐43. - PubMed
Tepe 2006
-
- Tepe G, Schmehl J, Heller S, Wiesinger B, Claussen CD, Duda SH. Superficial femoral artery: current treatment options. European Radiology 2006;16:1316‐22. - PubMed
Weaver 1996
-
- Weaver FA, Comerota AJ, Youngblood M, Froehlich J, Hosking JD, Papanicolaou G, STILE Investigators. Surgical revascularization versus thrombolysis for nonembolic lower extremity native artery occlusions: results of a prospective randomized trial. The STILE Investigators. Surgery versus Thrombolysis for Ischemia of the Lower Extremity. Journal of Vascular Surgery 1996;24(4):513‐23. - PubMed
References to other published versions of this review
Fowkes 2008
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous