

Risk of Thyroid Nodules in Residents of Belarus Exposed to Chernobyl Fallout as Children and Adolescents
- PMID: 28368520
- PMCID: PMC5505199
- DOI: 10.1210/jc.2016-3842
Risk of Thyroid Nodules in Residents of Belarus Exposed to Chernobyl Fallout as Children and Adolescents
Abstract
Context: Although radiation exposure is an important predictor of thyroid cancer on diagnosis of a thyroid nodule, the relationship between childhood radiation exposure and thyroid nodules has not been comprehensively evaluated.
Objective: To examine the association between internal I-131 thyroid dose and thyroid nodules in young adults exposed during childhood.
Design, setting, and participants: In this cross-sectional study, we screened residents of Belarus aged ≤18 years at the time of the Chernobyl nuclear accident for thyroid disease (median age, 21 years) with thyroid palpation, ultrasonography, blood/urine analysis, and medical follow-up when appropriate. Eligible participants (N = 11,421) had intact thyroid glands and doses based on direct individual thyroid activity measurements.
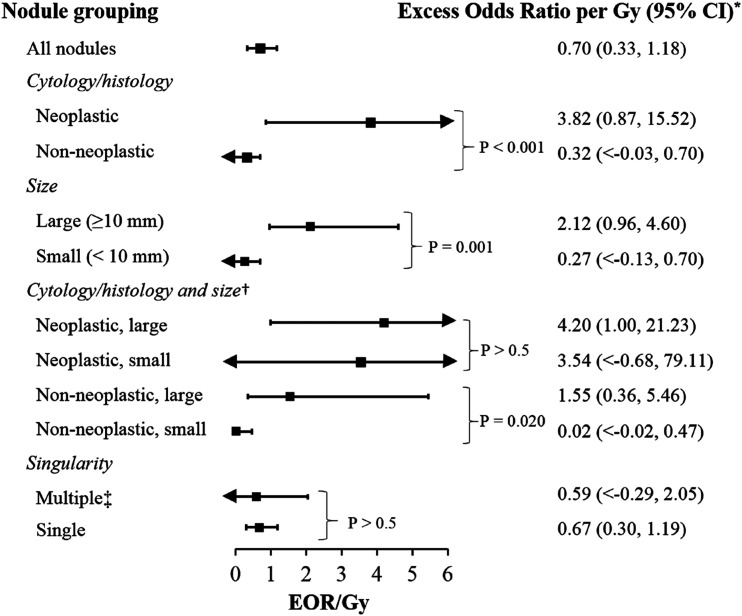
Main outcome measures: Excess odds ratios per Gray (EOR/Gy, scaled at age 5 years at exposure) for any thyroid nodule and for nodules grouped by cytology/histology, diameter size, and singularity.
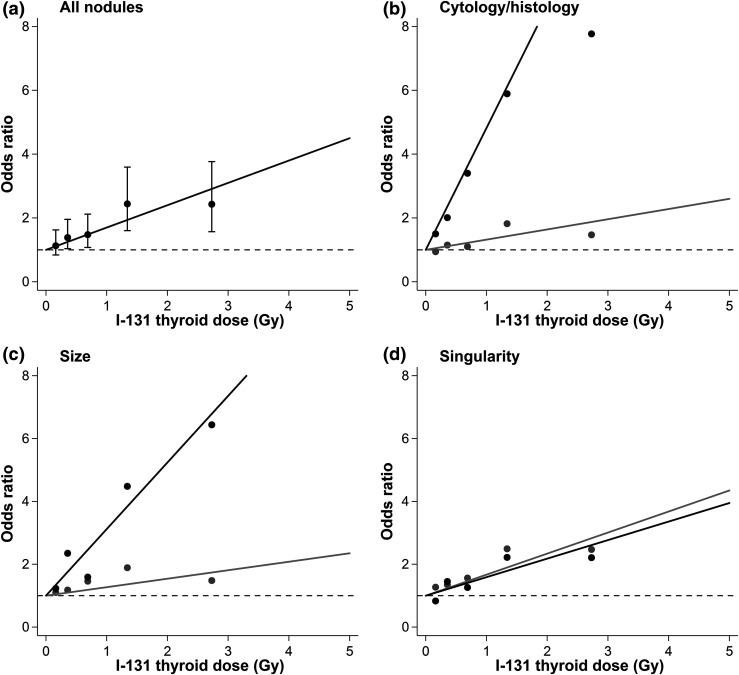
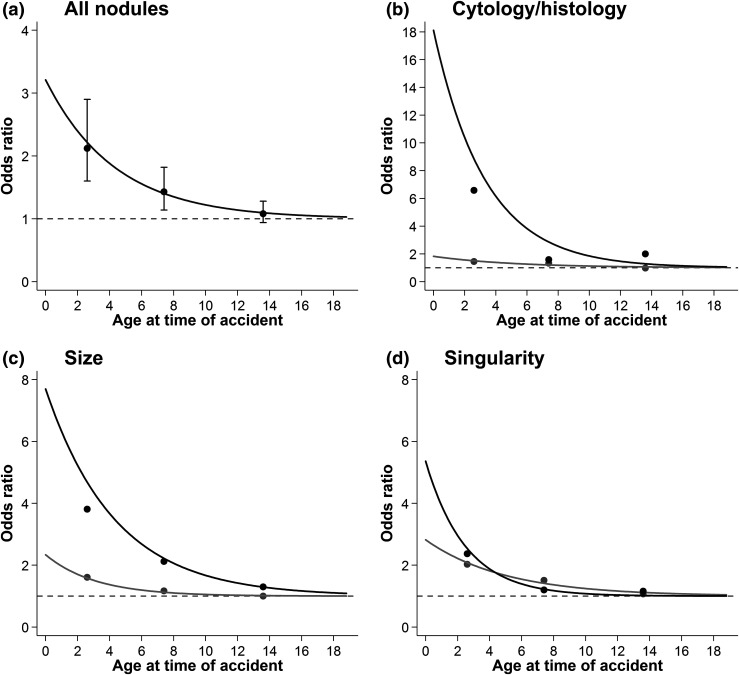
Results: Risk of any thyroid nodule increased significantly with I-131 dose and, for a given dose, with younger age at exposure. The EOR/Gy (95% confidence intervals) for neoplastic nodules (3.82; 0.87 to 15.52) was significantly higher than for nonneoplastic nodules (0.32; <0.03 to 0.70) and did not vary by size; whereas the EOR/Gy for nonneoplastic nodules did vary by size (P = 0.02) and was 1.55 (0.36 to 5.46) for nodules ≥10 mm and 0.02 (<-0.02 to 0.70) for nodules <10 mm. EORs/Gy for single and multiple nodules were comparable.
Conclusions: Childhood exposure to internal I-131 is associated with increased risk of neoplastic thyroid nodules of any size and nonneoplastic nodules ≥10 mm.
Copyright © 2017 Endocrine Society
Figures
Similar articles
-
Prevalence of Thyroid Nodules in Residents of Ukraine Exposed as Children or Adolescents to Iodine-131 from the Chornobyl Accident.Thyroid. 2024 Jul;34(7):890-898. doi: 10.1089/thy.2023.0654. Epub 2024 Jun 26. Thyroid. 2024. PMID: 38757581 Free PMC article.
-
Thyroid Cancer and Benign Nodules After Exposure In Utero to Fallout From Chernobyl.J Clin Endocrinol Metab. 2019 Jan 1;104(1):41-48. doi: 10.1210/jc.2018-00847. J Clin Endocrinol Metab. 2019. PMID: 30445441 Free PMC article.
-
Thyroid cancer risk in Belarus among children and adolescents exposed to radioiodine after the Chornobyl accident.Br J Cancer. 2011 Jan 4;104(1):181-7. doi: 10.1038/sj.bjc.6605967. Epub 2010 Nov 23. Br J Cancer. 2011. PMID: 21102590 Free PMC article.
-
Radioactivity and thyroid cancer.Hormones (Athens). 2009 Jul-Sep;8(3):185-91. doi: 10.14310/horm.2002.1234. Hormones (Athens). 2009. PMID: 19671517 Review.
-
[The effect of Chernobyl accident on the development of malignant diseases--situation after 20 years].Endokrynol Pol. 2006 May-Jun;57(3):244-52. Endokrynol Pol. 2006. PMID: 16832789 Review. Polish.
Cited by
-
Thyroid Cancer in Kazakhstan: Component Analysis of Incidence Dynamics.Asian Pac J Cancer Prev. 2019 Sep 1;20(9):2875-2880. doi: 10.31557/APJCP.2019.20.9.2875. Asian Pac J Cancer Prev. 2019. PMID: 31554390 Free PMC article.
-
Contemporary Thyroid Nodule Evaluation and Management.J Clin Endocrinol Metab. 2020 Sep 1;105(9):2869-83. doi: 10.1210/clinem/dgaa322. J Clin Endocrinol Metab. 2020. PMID: 32491169 Free PMC article. Review.
-
Elemental comparative analysis of 18 elements reveal distinct patterns in benign and malignant thyroid tissues.Biometals. 2025 Jun;38(3):873-886. doi: 10.1007/s10534-025-00682-w. Epub 2025 Apr 29. Biometals. 2025. PMID: 40299266
-
Risk of Benign and Malignant Thyroid Disorders in Subjects Treated for Paediatric/Adolescent Neoplasia: Role of Morphological and Functional Screening.Children (Basel). 2021 Aug 31;8(9):767. doi: 10.3390/children8090767. Children (Basel). 2021. PMID: 34572198 Free PMC article.
-
Radiation Exposure to the Thyroid After the Chernobyl Accident.Front Endocrinol (Lausanne). 2021 Jan 5;11:569041. doi: 10.3389/fendo.2020.569041. eCollection 2020. Front Endocrinol (Lausanne). 2021. PMID: 33469445 Free PMC article. Review.
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. - PMC - PubMed
-
- Hegedüs L. Clinical practice: the thyroid nodule. N Engl J Med. 2004;351(17):1764–1771. - PubMed
-
- Singer PA, Cooper DS, Daniels GH, Ladenson PW, Greenspan FS, Levy EG, Braverman LE, Clark OH, McDougall IR, Ain KV, Dorfman SG; American Thyroid Association . Treatment guidelines for patients with thyroid nodules and well-differentiated thyroid cancer. Arch Intern Med. 1996;156(19):2165–2172. - PubMed
-
- Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, Panunzi C, Rinaldi R, Toscano V, Pacella CM. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002;87(5):1941–1946. - PubMed
-
- Acharya S, Sarafoglou K, LaQuaglia M, Lindsley S, Gerald W, Wollner N, Tan C, Sklar C. Thyroid neoplasms after therapeutic radiation for malignancies during childhood or adolescence. Cancer. 2003;97(10):2397–2403. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
