

Risk of Acute Coronary Heart Disease After Sepsis Hospitalization in the REasons for Geographic and Racial Differences in Stroke (REGARDS) Cohort
- PMID: 28369197
- PMCID: PMC5849104
- DOI: 10.1093/cid/cix248
Risk of Acute Coronary Heart Disease After Sepsis Hospitalization in the REasons for Geographic and Racial Differences in Stroke (REGARDS) Cohort
Abstract
Background: Sepsis is associated with long-term health consequences. We sought to determine the long-term risks of acute and fatal coronary heart disease (CHD) events after sepsis hospitalizations among community-dwelling adults.
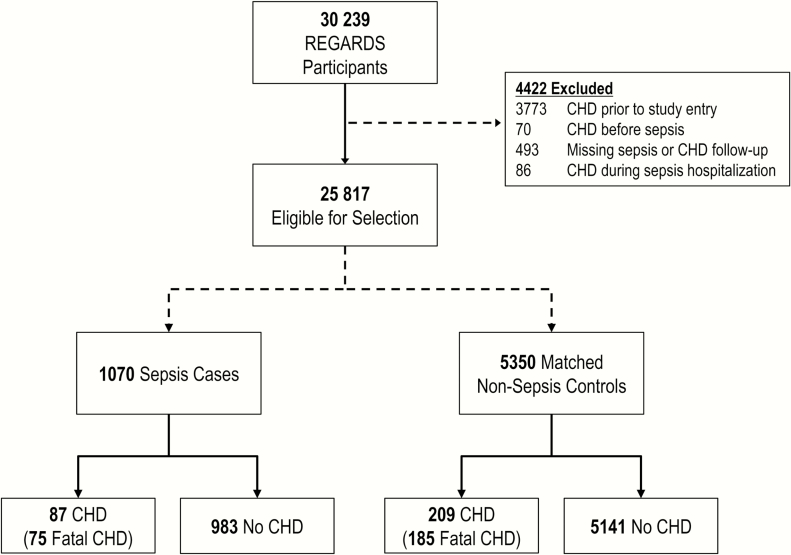
Methods: We analyzed data from 30329 participants in the population-based REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort. Sepsis events included hospitalizations for a serious infection with ≥2 systemic inflammatory response syndrome criteria. Acute CHD events included myocardial infarctions (MIs; nonfatal and fatal) and acute CHD deaths. Fatal CHD included deaths ≤28 days of an acute MI and acute CHD deaths. We age- and time-matched each sepsis participant with 5 nonsepsis participants. We assessed the associations between sepsis hospitalizations and future acute and fatal CHD events using Cox regression, Gray's model, and competing risks analysis, adjusting for comorbidities.
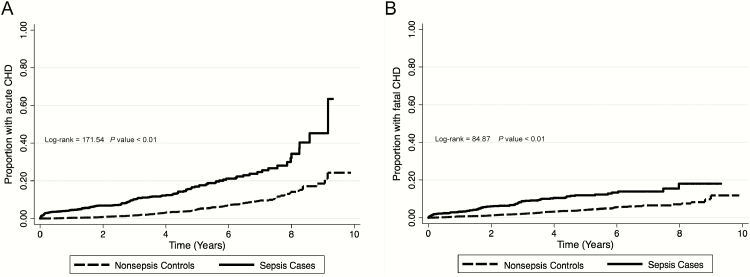
Results: The matched cohort contained 1070 sepsis and 5350 nonsepsis participants. Risk of acute CHD was higher for sepsis than nonsepsis controls after adjusting for sex, race, education, income, region, tobacco use, and select chronic medical conditions (0-1 year adjusted hazard ratio [HR], 4.38 [95% confidence interval (CI), 2.03-9.45]; 1-4 years, 1.78 [1.09-2.88]; and 4+ years, 1.18 [0.52-2.67]). Risk of fatal CHD was similarly higher for sepsis than nonsepsis individuals (0-1 year adjusted HR, 3.12 [95% CI, 1.35-7.23]; 1-4 years, 3.29 [1.89-5.74]; and 4+ years HR, 1.15 [0.34-3.94]).
Conclusions: The long-term risks of acute and fatal CHD are elevated after sepsis hospitalization. Management of acute CHD risk may be important for individuals surviving a sepsis event.
Keywords: epidemiology; heart disease; infections; myocardial infarction; sepsis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29:1303–10. - PubMed
-
- Winters BD, Eberlein M, Leung J, Needham DM, Pronovost PJ, Sevransky JE. Long-term mortality and quality of life in sepsis: a systematic review. Crit Care Med 2010; 38:1276–83. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
