

Implications of Antibiotic Resistance for Patients' Recovery From Common Infections in the Community: A Systematic Review and Meta-analysis
- PMID: 28369247
- PMCID: PMC5850316
- DOI: 10.1093/cid/cix233
Implications of Antibiotic Resistance for Patients' Recovery From Common Infections in the Community: A Systematic Review and Meta-analysis
Abstract
Background: Antibiotic use is the main driver for carriage of antibiotic-resistant bacteria. The perception exists that failure of antibiotic treatment due to antibiotic resistance has little clinical impact in the community.
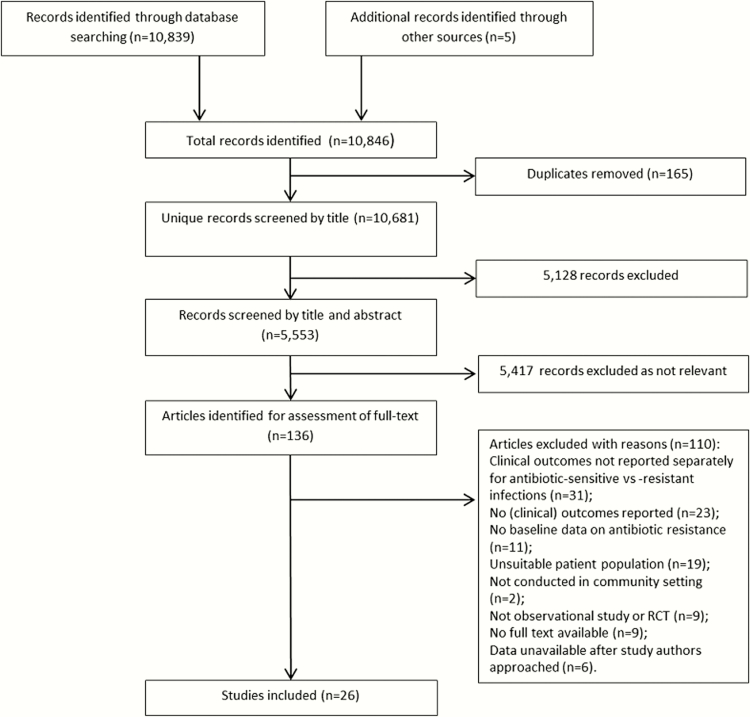
Methods: We searched MEDLINE, EMBASE, PubMed, Cochrane Central Register of Controlled Trials, and Web of Science from inception to 15 April 2016 without language restriction. We included studies conducted in community settings that reported patient-level data on laboratory-confirmed infections (respiratory tract, urinary tract, skin or soft tissue), antibiotic resistance, and clinical outcomes. Our primary outcome was clinical response failure. Secondary outcomes were reconsultation, further antibiotic prescriptions, symptom duration, and symptom severity. Where possible, we calculated odds ratios with 95% confidence intervals by performing meta-analysis using random effects models.
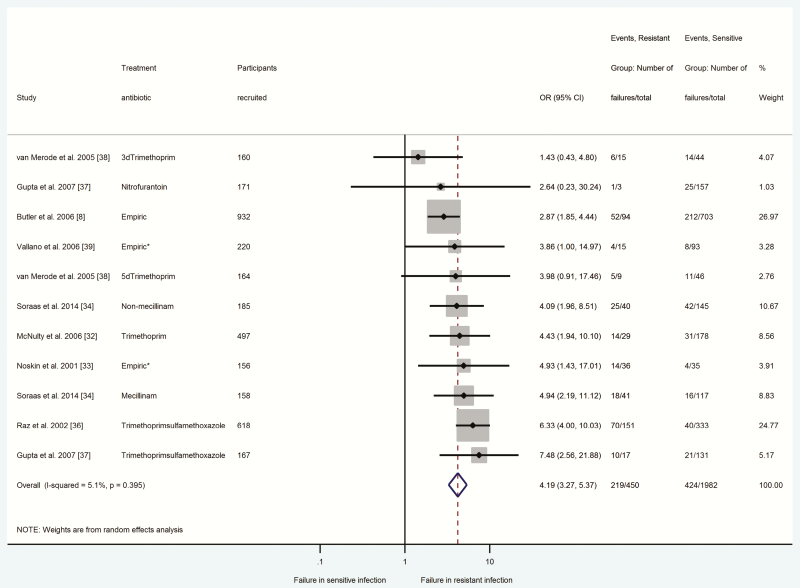
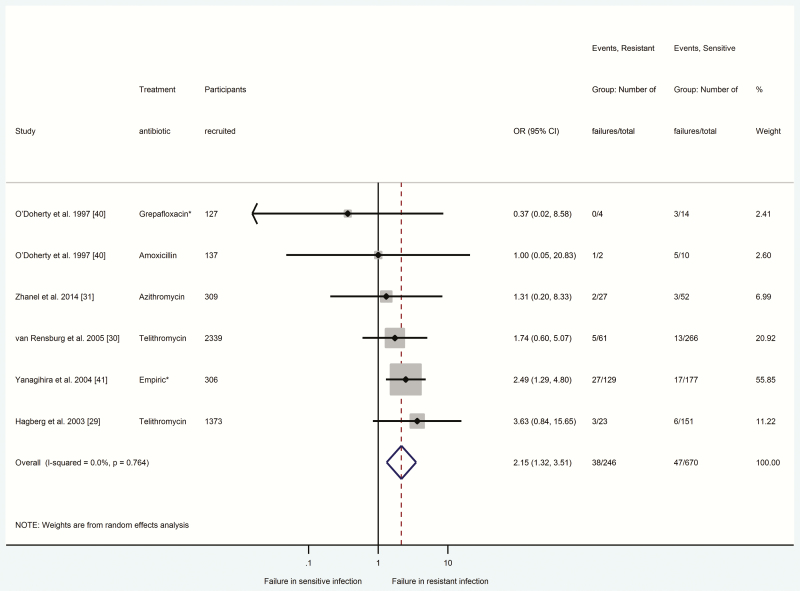
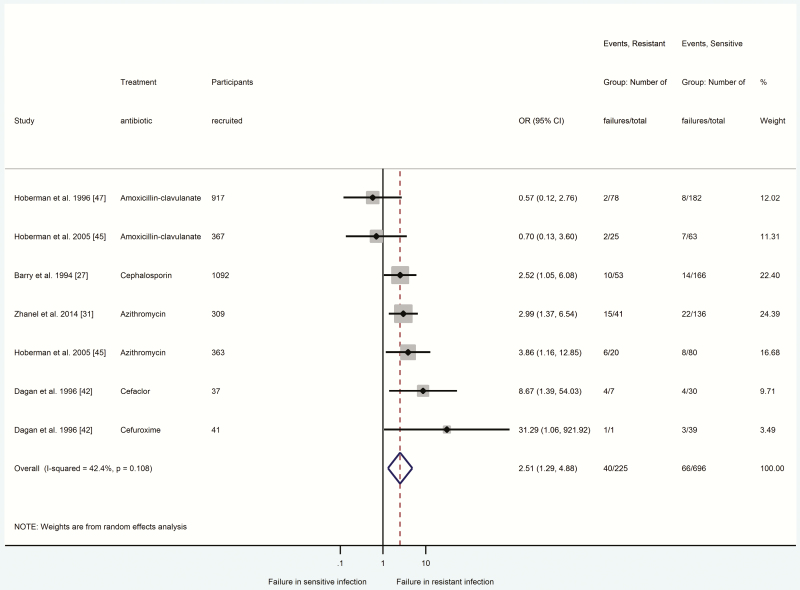
Results: We included 26 studies (5659 participants). Clinical response failure was significantly more likely in participants with antibiotic-resistant Escherichia coli urinary tract infections (odds ratio [OR] = 4.19; 95% confidence interval [CI] = 3.27-5.37; n = 2432 participants), Streptococcus pneumoniae otitis media (OR = 2.51; 95% CI = 1.29-4.88; n = 921 participants), and S. pneumoniae community-acquired pneumonia (OR = 2.15; 95% CI = 1.32-3.51; n = 916 participants). Clinical heterogeneity precluded primary outcome meta-analysis for Staphylococcus aureus skin or soft-tissue infections.
Conclusions: Antibiotic resistance significantly impacts on patients' illness burden in the community. Patients with laboratory-confirmed antibiotic-resistant urinary and respiratory-tract infections are more likely to experience delays in clinical recovery after treatment with antibiotics. A better grasp of the risk of antibiotic resistance on outcomes that matter to patients should inform more meaningful discussions between healthcare professionals and patients about antibiotic treatment for common infections.
Keywords: antibiotic resistance; clinical significance; primary care.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com
Figures
References
-
- Simpson SA, Wood F, Butler CC. General practitioners’ perceptions of antimicrobial resistance: a qualitative study. J Antimicrob Chemother 2007; 59:292–6. - PubMed
-
- McCullough AR, Parekh S, Rathbone J, Del Mar CB, Hoffmann TC. A systematic review of the public’s knowledge and beliefs about antibiotic resistance. J Antimicrob Chemother 2016; 71:27–33. - PubMed
-
- Wood F, Simpson S, Butler CC. Socially responsible antibiotic choices in primary care: a qualitative study of GPs’ decisions to prescribe broad-spectrum and fluroquinolone antibiotics. Fam Pract 2007; 24:427–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
