

Gastrointestinal Carriage Is a Major Reservoir of Klebsiella pneumoniae Infection in Intensive Care Patients
- PMID: 28369261
- PMCID: PMC5850561
- DOI: 10.1093/cid/cix270
Gastrointestinal Carriage Is a Major Reservoir of Klebsiella pneumoniae Infection in Intensive Care Patients
Abstract
Background: Klebsiella pneumoniae is an opportunistic pathogen and leading cause of hospital-associated infections. Intensive care unit (ICU) patients are particularly at risk. Klebsiella pneumoniae is part of the healthy human microbiome, providing a potential reservoir for infection. However, the frequency of gut colonization and its contribution to infections are not well characterized.
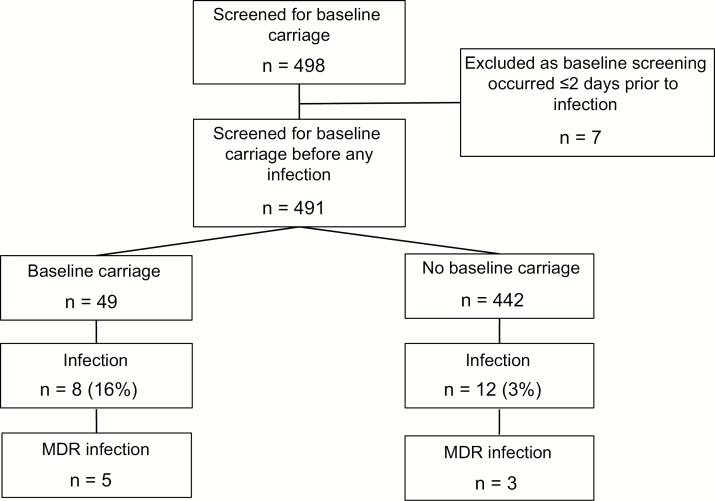
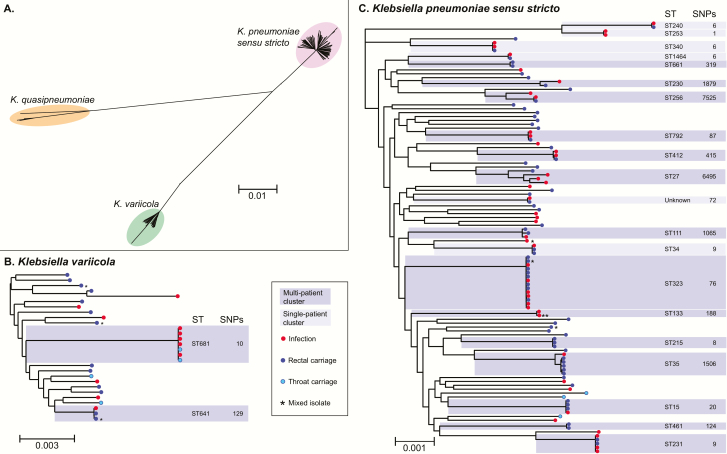
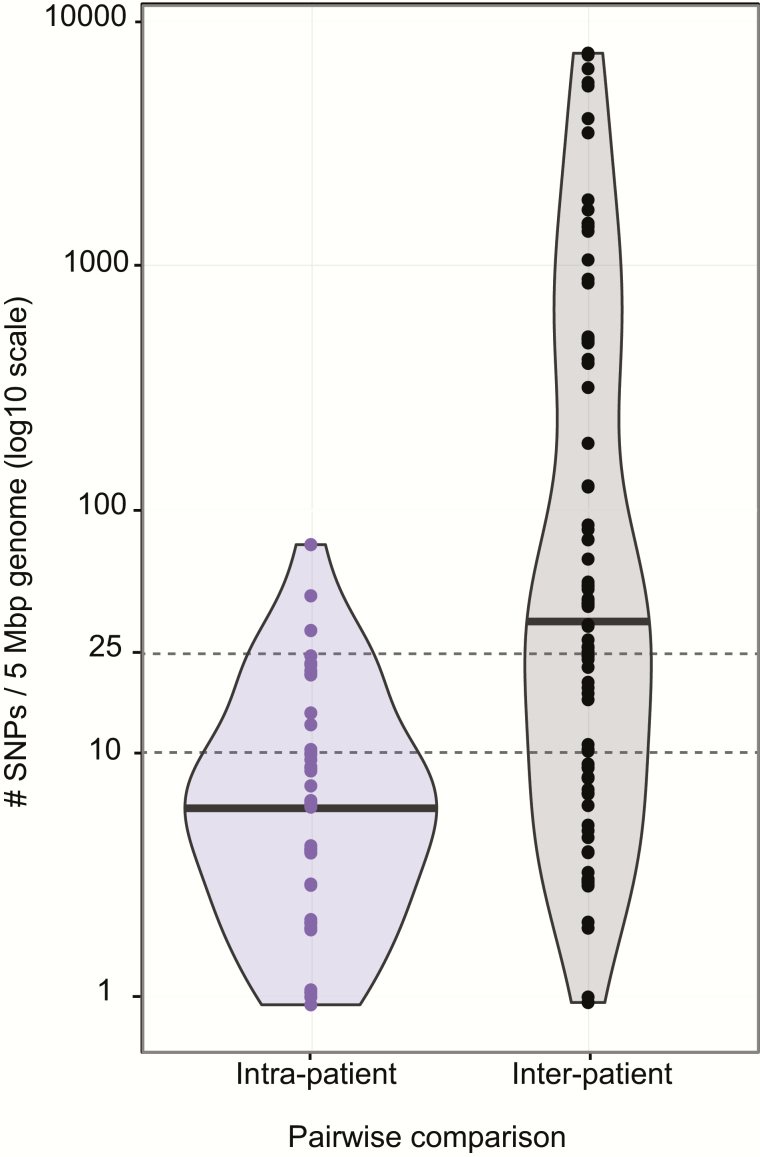
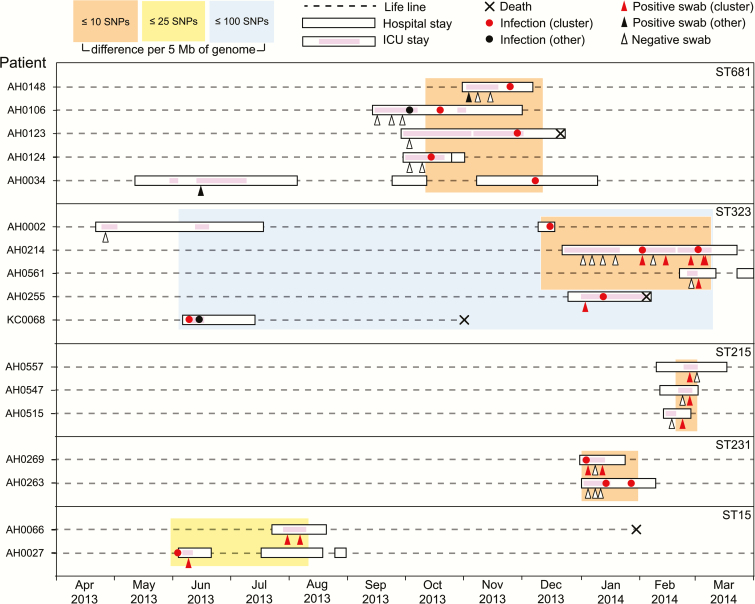
Methods: We conducted a 1-year prospective cohort study in which 498 ICU patients were screened for rectal and throat carriage of K. pneumoniae shortly after admission. Klebsiella pneumoniae isolated from screening swabs and clinical diagnostic samples were characterized using whole genome sequencing and combined with epidemiological data to identify likely transmission events.
Results: Klebsiella pneumoniae carriage frequencies were estimated at 6% (95% confidence interval [CI], 3%-8%) among ICU patients admitted direct from the community, and 19% (95% CI, 14%-51%) among those with recent healthcare contact. Gut colonization on admission was significantly associated with subsequent infection (infection risk 16% vs 3%, odds ratio [OR] = 6.9, P < .001), and genome data indicated matching carriage and infection isolates in 80% of isolate pairs. Five likely transmission chains were identified, responsible for 12% of K. pneumoniae infections in ICU. In sum, 49% of K. pneumoniae infections were caused by the patients' own unique strain, and 48% of screened patients with infections were positive for prior colonization.
Conclusions: These data confirm K. pneumoniae colonization is a significant risk factor for infection in ICU, and indicate ~50% of K. pneumoniae infections result from patients' own microbiota. Screening for colonization on admission could limit risk of infection in the colonized patient and others.
Keywords: Klebsiella pneumoniae; gastrointestinal colonization; genomic epidemiology; hospital acquired infection; intensive care.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Genome watch: Klebsiella pneumoniae: when a colonizer turns bad.Nat Rev Microbiol. 2017 Jul;15(7):384. doi: 10.1038/nrmicro.2017.64. Epub 2017 Jun 5. Nat Rev Microbiol. 2017. PMID: 28579608 No abstract available.
References
-
- Centres for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013: Centres for Disease Control and Prevention, US Department of Health and Human Services, 2013.
-
- Paterson DL, Ko WC, Von Gottberg A, et al. Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of production of extended-spectrum beta-lactamases. Clin Infect Dis 2004; 39:31–7. - PubMed
-
- Wiener-Well Y, Rudensky B, Yinnon AM, et al. Carriage rate of carbapenem-resistant Klebsiella pneumoniae in hospitalised patients during a national outbreak. J Hosp Infect 2010; 74:344–9. - PubMed
-
- Peña C, Pujol M, Ricart A, et al. Risk factors for faecal carriage of Klebsiella pneumoniae producing extended spectrum beta-lactamase (ESBL-KP) in the intensive care unit. J Hosp Infect 1997; 35:9–16. - PubMed
-
- Weinstein RA, Gaynes R, Edwards JR; National Nosocomial Infections Surveillance System Overview of nosocomial infections caused by gram-negative bacilli. Clin Infect Dis 2005; 41:848–54. - PubMed
