

Klinefelter syndrome comorbidities linked to increased X chromosome gene dosage and altered protein interactome activity
- PMID: 28369266
- PMCID: PMC5390676
- DOI: 10.1093/hmg/ddx014
Klinefelter syndrome comorbidities linked to increased X chromosome gene dosage and altered protein interactome activity
Abstract
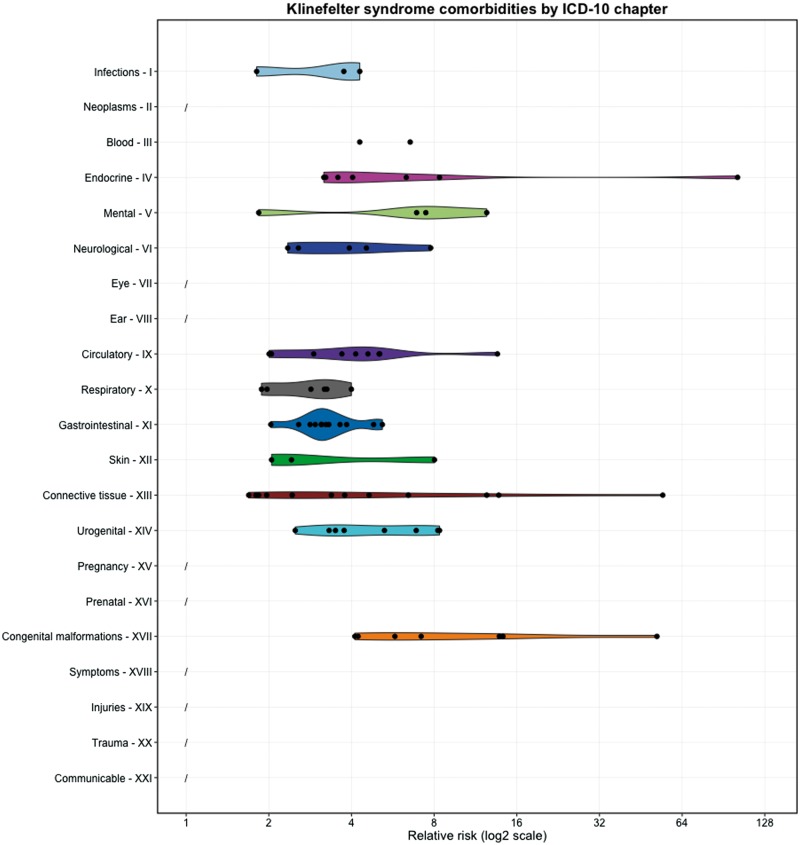
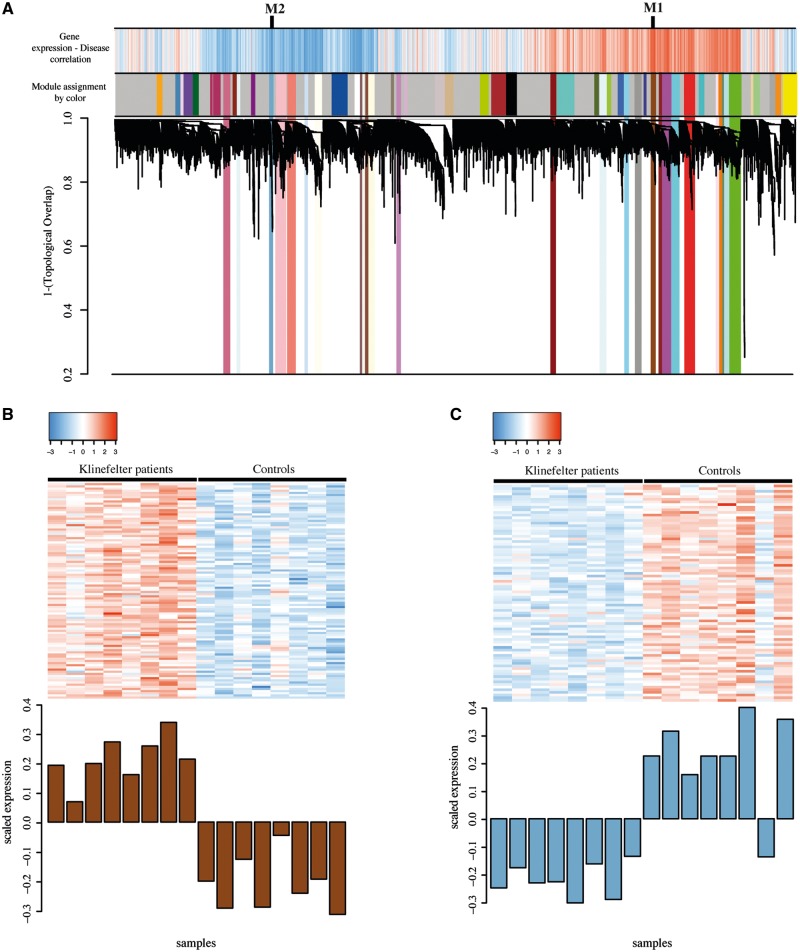
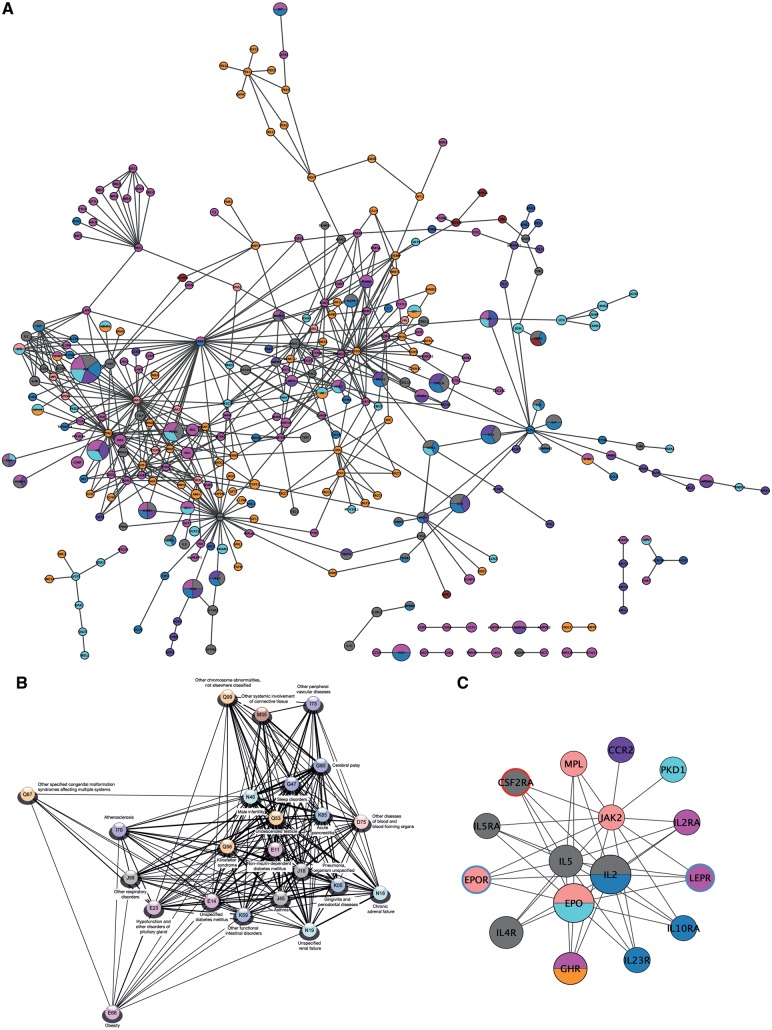
Klinefelter syndrome (KS) (47,XXY) is the most common male sex chromosome aneuploidy. Diagnosis and clinical supervision remain a challenge due to varying phenotypic presentation and insufficient characterization of the syndrome. Here we combine health data-driven epidemiology and molecular level systems biology to improve the understanding of KS and the molecular interplay influencing its comorbidities. In total, 78 overrepresented KS comorbidities were identified using in- and out-patient registry data from the entire Danish population covering 6.8 million individuals. The comorbidities extracted included both clinically well-known (e.g. infertility and osteoporosis) and still less established KS comorbidities (e.g. pituitary gland hypofunction and dental caries). Several systems biology approaches were applied to identify key molecular players underlying KS comorbidities: Identification of co-expressed modules as well as central hubs and gene dosage perturbed protein complexes in a KS comorbidity network build from known disease proteins and their protein-protein interactions. The systems biology approaches together pointed to novel aspects of KS disease phenotypes including perturbed Jak-STAT pathway, dysregulated genes important for disturbed immune system (IL4), energy balance (POMC and LEP) and erythropoietin signalling in KS. We present an extended epidemiological study that links KS comorbidities to the molecular level and identify potential causal players in the disease biology underlying the identified comorbidities.
© The Author 2017. Published by Oxford University Press.
Figures
References
-
- Bojesen A., Juul S., Gravholt C.H. (2003) Prenatal and postnatal prevalence of Klinefelter syndrome: a national registry study. J. Clin. Endocrinol. Metab., 88, 622–626. - PubMed
-
- Dürrbaum M., Storchova Z. (2016) Effects of aneuploidy on gene expression: implications for cancer. FEBS J., 283, 791–802. - PubMed
-
- Kirk, I. K., Weinhold, N., Belling, K., Skakkebæk, N. E., Jensen, T. S., Leffers, H., Juul, A. and Brunak, S. (2017) Chromosome-wise protein interaction patterns and their impact on functional implications of large-scale genomic aberrations. Cell Systems, 4, 1–8. - PubMed
-
- Lanfranco F., Kamischke A., Zitzmann M., Nieschlag E. (2004) Klinefelter's syndrome. Lancet, 364, 273–283. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
