

Chimerism-based tolerance in organ transplantation: preclinical and clinical studies
- PMID: 28369830
- PMCID: PMC5508349
- DOI: 10.1111/cei.12969
Chimerism-based tolerance in organ transplantation: preclinical and clinical studies
Abstract
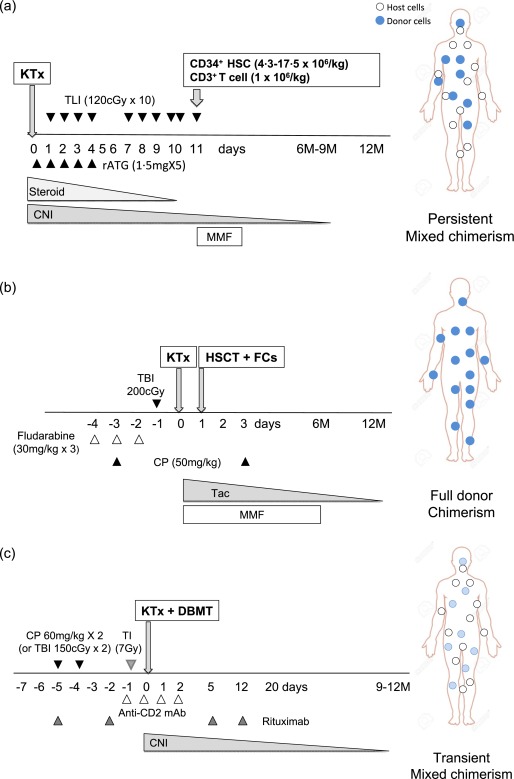
Induction of allograft tolerance has been considered the ultimate goal in organ transplantation. Although numerous protocols to induce allograft tolerance have been reported in mice, a chimerism-based approach through donor haematopoietic stem cell transplantation has been the only approach to date that induced allograft tolerance reproducibly following kidney transplantation in man. Renal allograft tolerance has been achieved by induction of either transient mixed chimerism or persistent full donor chimerism. Although the risk of rejection may be low in tolerance achieved via durable full donor chimerism, the development of graft-versus-host disease (GVHD) has limited the wider clinical application of this approach. In contrast, tolerance induced by transient mixed chimerism has not been associated with GVHD, but the risk of allograft rejection is more difficult to predict after the disappearance of haematopoietic chimerism. Current efforts are directed towards the development of more clinically feasible and reliable approaches to induce more durable mixed chimerism in order to widen the clinical applicability of these treatment regimens.
Keywords: GVHD; NHP; TBI; TI; TLI; chimerism; cyclophosphamide; durable mixed chimerism; full donor chimerism; haematopoietic stem cell transplantation; living-donor kidney transplantation; persistent mixed chimerism; transient mixed chimerism; transplantation tolerance induction.
© 2017 British Society for Immunology.
Figures
References
-
- Meier‐Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 2004; 4:378–83. - PubMed
-
- Lodhi SA, Lamb KE, Meier‐Kriesche HU. Solid organ allograft survival improvement in the United States: the long‐term does not mirror the dramatic short‐term success. Am J Transplant 2011; 11:1226–35. - PubMed
-
- Miller LW. Cardiovascular toxicities of immunosuppressive agents. Am J Transplant 2002; 2:807–18. - PubMed
-
- Lentine KL, Brennan DC, Schnitzler MA. Incidence and predictors of myocardial infarction after kidney transplantation. J Am Soc Nephrol 2005; 16:496–506. - PubMed
-
- Morales JM, Dominguez‐Gil B. Cardiovascular risk profile with the new immunosuppressive combinations after renal transplantation. J Hypertens 2005; 23:1609–16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
