

Changes in chondrolabral mechanics, coverage, and congruency following peri-acetabular osteotomy for treatment of acetabular retroversion: A patient-specific finite element study
- PMID: 28370312
- PMCID: PMC5623608
- DOI: 10.1002/jor.23566
Changes in chondrolabral mechanics, coverage, and congruency following peri-acetabular osteotomy for treatment of acetabular retroversion: A patient-specific finite element study
Abstract
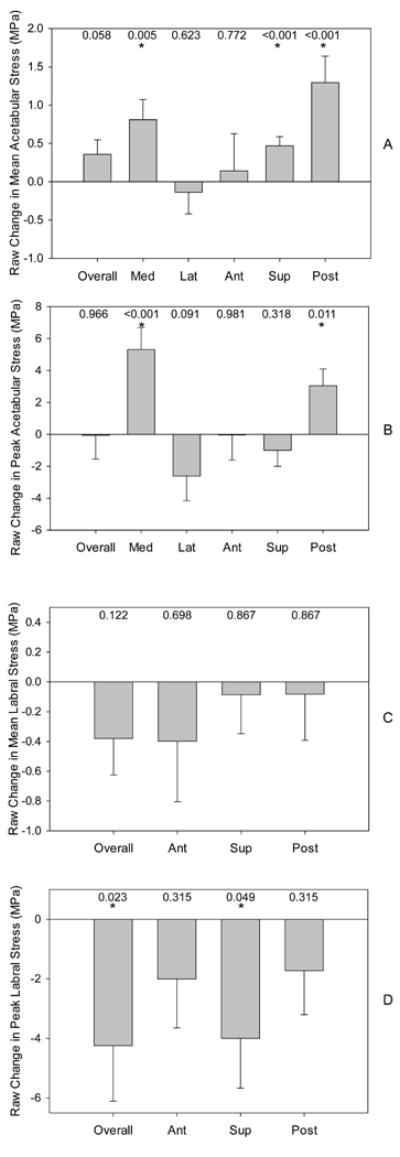
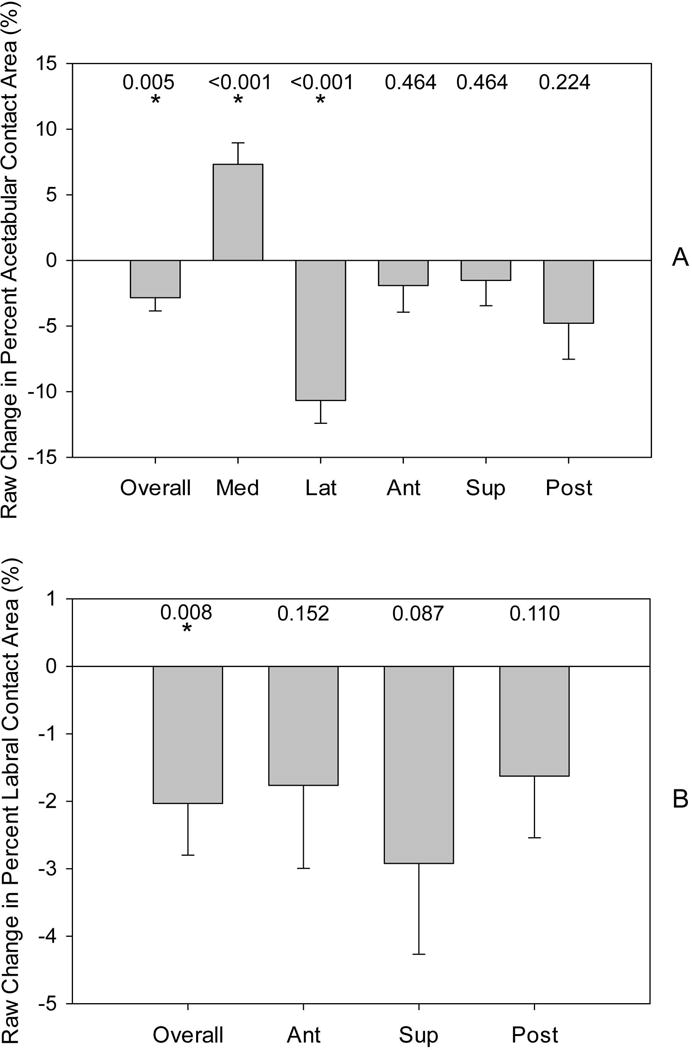
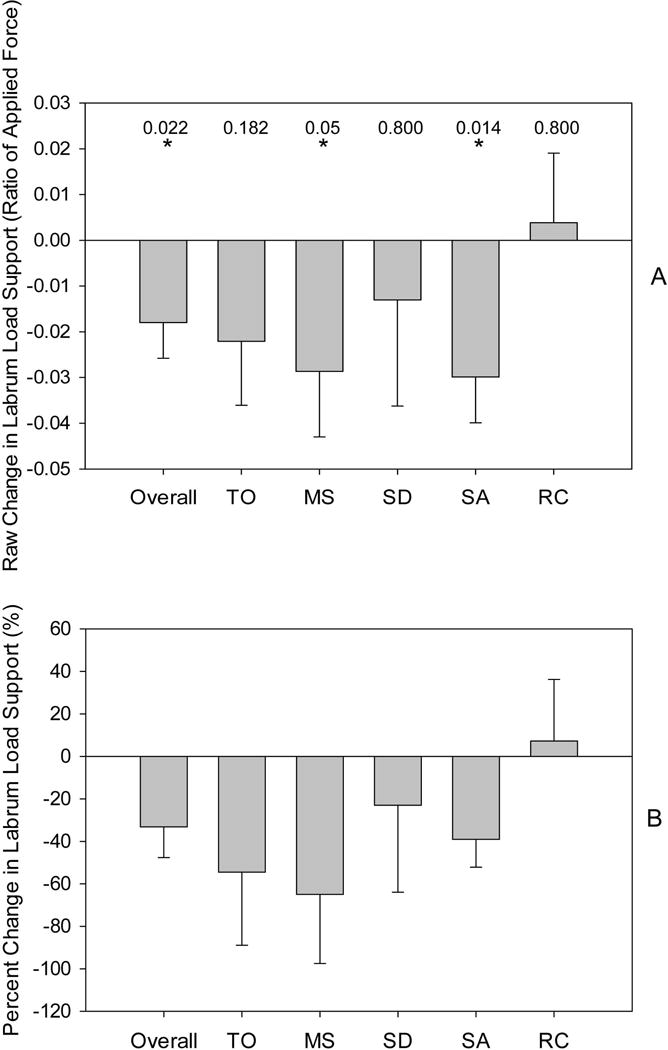
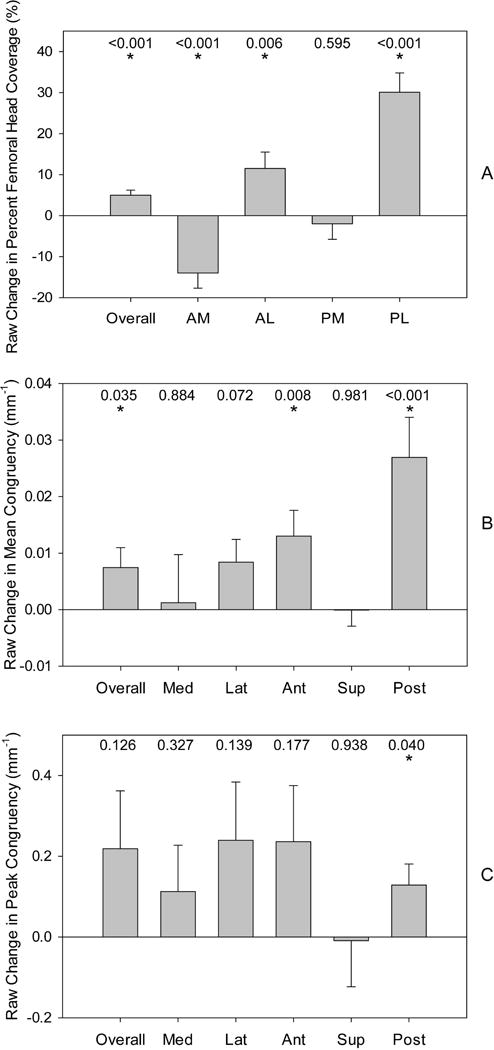
Using a validated finite element (FE) protocol, we quantified cartilage and labrum mechanics, congruency, and femoral coverage in five male patients before and after they were treated for acetabular retroversion with peri-acetabular osteotomy (PAO). Three-dimensional models of bone, cartilage, and labrum were generated from computed tomography (CT) arthrography images, acquired before and after PAO. Walking, stair-ascent, stair-descent, and rising from a chair were simulated. Cartilage and labrum contact stress, contact area, and femoral coverage were calculated overall and regionally. Mean congruency (average of local congruency values for FE nodes in contact) and peak congruency (most incongruent node in contact) were calculated overall and regionally. Load supported by the labrum was represented as a raw change in the ratio of the applied force transferred through the labrum and percent change following surgery (calculated overall only). Considering all activities, following PAO, mean acetabular cartilage contact stress increased medially, superiorly, and posteriorly; peak stress increased medially and posteriorly. Peak labrum stresses decreased overall and superiorly. Acetabular contact area decreased overall and laterally, and increased medially. Labral contact area decreased overall, but not regionally. Load to the labrum decreased. Femoral head coverage increased overall, anterolaterally, and posterolaterally, but decreased anteromedially. Mean congruency indicated the hip became less congruent overall, anteriorly, and posteriorly; peak congruency indicated a less congruent joint posteriorly.
Clinical relevance: Medialization of contact and reductions in labral loading following PAO may prevent osteoarthritis, but this procedure increases cartilage stresses, decreases contact area, and makes the hip less congruent, which may overload cartilage. © 2017 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res 35:2567-2576, 2017.
Keywords: chondrolabral mechanics; finite element analysis; hip; morphology; retroversion.
© 2017 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
Conflict of interest statement
Figures
References
-
- Ezoe M, Naito M, Inoue T. The prevalence of acetabular retroversion among various disorders of the hip. J Bone Joint Surg Am. 2006;88:372–379. - PubMed
-
- Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999;81:281–288. - PubMed
-
- Dandachli W, Islam SU, Liu M, et al. Three-dimensional CT analysis to determine acetabular retroversion and the implications for the management of femoro-acetabular impingement. J Bone Joint Surg Br. 2009;91:1031–1036. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
