

Regeneration of injured skin and peripheral nerves requires control of wound contraction, not scar formation
- PMID: 28370669
- PMCID: PMC5520812
- DOI: 10.1111/wrr.12516
Regeneration of injured skin and peripheral nerves requires control of wound contraction, not scar formation
Abstract
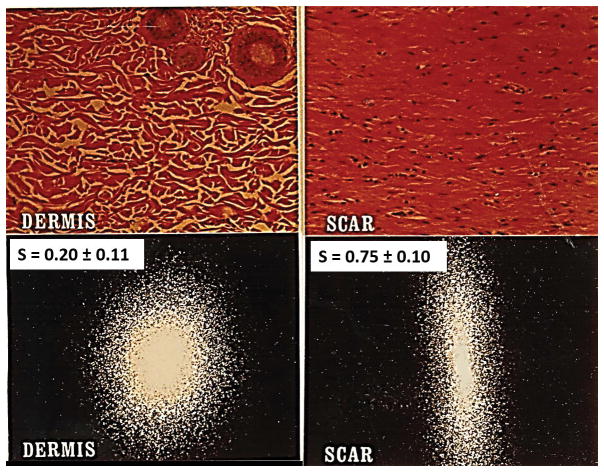
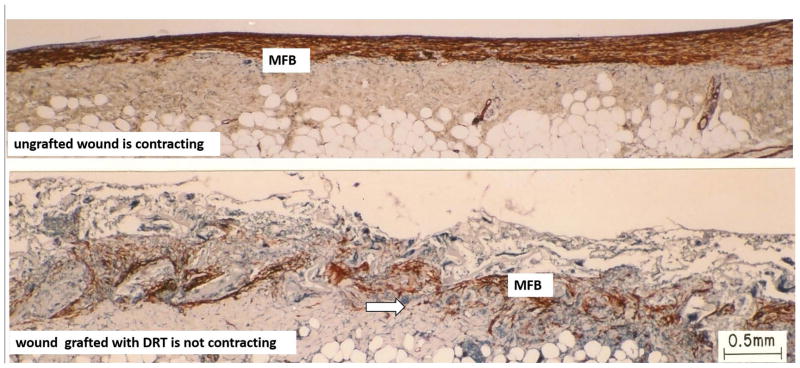
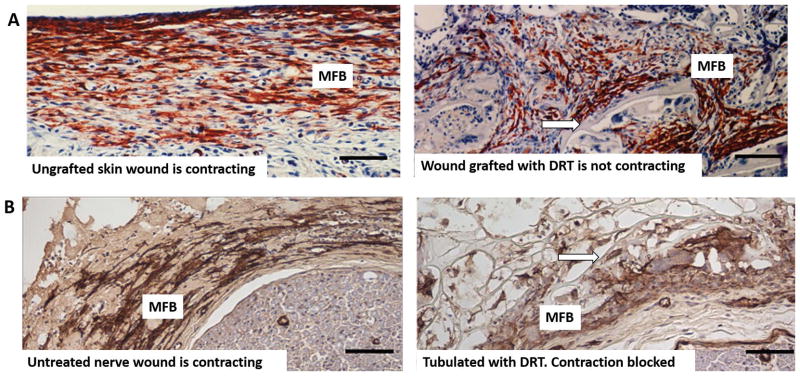
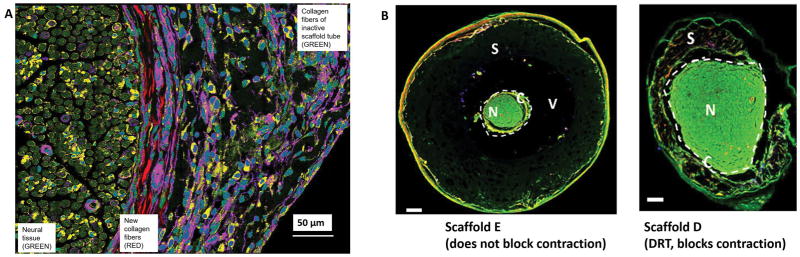
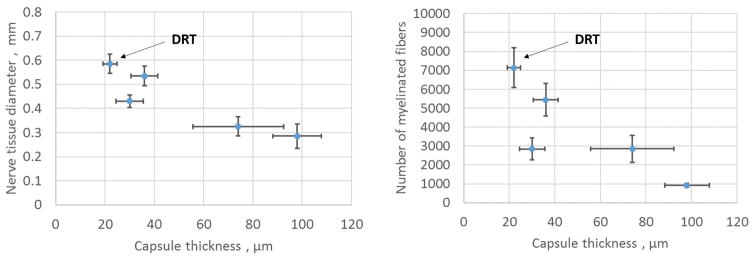
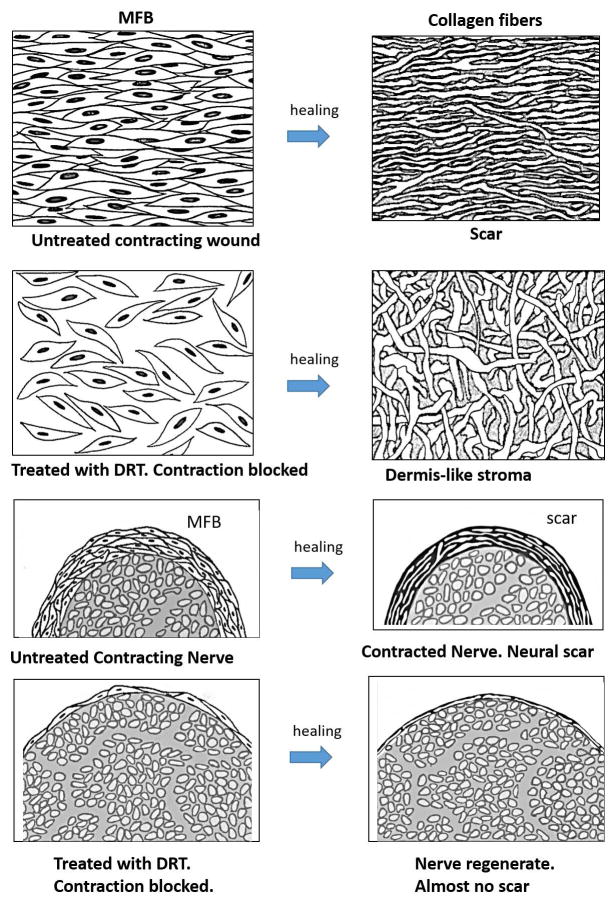
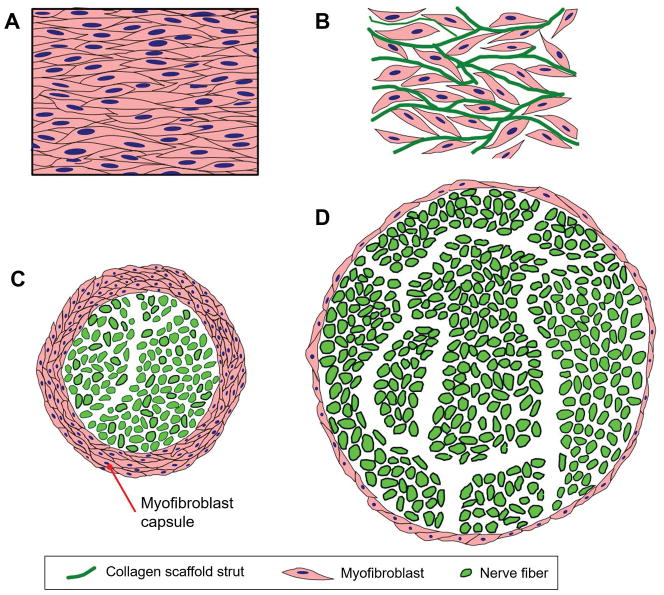
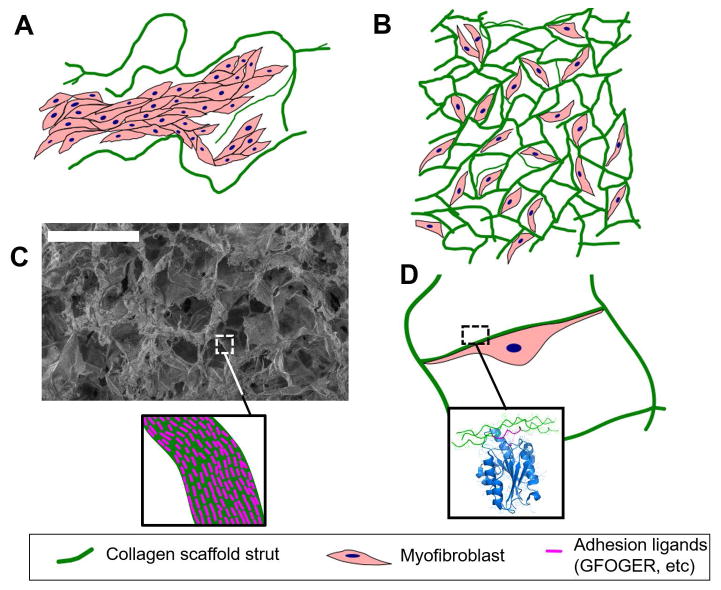
We review the mounting evidence that regeneration is induced in wounds in skin and peripheral nerves by a simple modification of the wound healing process. Here, the process of induced regeneration is compared to the other two well-known processes by which wounds close, i.e., contraction and scar formation. Direct evidence supports the hypothesis that the mechanical force of contraction (planar in skin wounds, circumferential in nerve wounds) is the driver guiding the orientation of assemblies of myofibroblasts (MFB) and collagen fibers during scar formation in untreated wounds. We conclude that scar formation depends critically on wound contraction and is, therefore, a healing process secondary to contraction. Wound contraction and regeneration did not coincide during healing in a number of experimental models of spontaneous (untreated) regeneration described in the literature. Furthermore, in other studies in which an efficient contraction-blocker, a collagen scaffold named dermis regeneration template (DRT), and variants of it, were grafted on skin wounds or peripheral nerve wounds, regeneration was systematically observed in the absence of contraction. We conclude that contraction and regeneration are mutually antagonistic processes. A dramatic change in the phenotype of MFB was observed when the contraction-blocking scaffold DRT was used to treat wounds in skin and peripheral nerves. The phenotype change was directly observed as drastic reduction in MFB density, dispersion of MFB assemblies and loss of alignment of the long MFB axes. These observations were explained by the evidence of a surface-biological interaction of MFB with the scaffold, specifically involving binding of MFB integrins α1 β1 and α2 β1 to ligands GFOGER and GLOGER naturally present on the surface of the collagen scaffold. In summary, we show that regeneration of wounded skin and peripheral nerves in the adult mammal can be induced simply by appropriate control of wound contraction, rather than of scar formation.
© 2017 by the Wound Healing Society.
Conflict of interest statement
Conflict statement
I.V. Yannas has participated in the founding of Integra LifeSciences, Plainsboro, NJ. He currently has no financial connection with the company and owns no stock of Integra LifeSciences.
Figures
Similar articles
-
Surface biology of collagen scaffold explains blocking of wound contraction and regeneration of skin and peripheral nerves.Biomed Mater. 2015 Dec 23;11(1):014106. doi: 10.1088/1748-6041/11/1/014106. Biomed Mater. 2015. PMID: 26694657 Free PMC article. Review.
-
Regeneration mechanism for skin and peripheral nerves clarified at the organ and molecular scales.Curr Opin Biomed Eng. 2018 Jun;6:1-7. doi: 10.1016/j.cobme.2017.12.002. Curr Opin Biomed Eng. 2018. PMID: 29392187 Free PMC article.
-
Common features of optimal collagen scaffolds that disrupt wound contraction and enhance regeneration both in peripheral nerves and in skin.Biomaterials. 2012 Jun;33(19):4783-91. doi: 10.1016/j.biomaterials.2012.03.068. Epub 2012 Apr 6. Biomaterials. 2012. PMID: 22483241
-
Modulation of scar tissue formation using different dermal regeneration templates in the treatment of experimental full-thickness wounds.Wound Repair Regen. 2004 Sep-Oct;12(5):518-27. doi: 10.1111/j.1067-1927.2004.012504.x. Wound Repair Regen. 2004. PMID: 15453834
-
Mammals fail to regenerate organs when wound contraction drives scar formation.NPJ Regen Med. 2021 Jul 22;6(1):39. doi: 10.1038/s41536-021-00149-9. NPJ Regen Med. 2021. PMID: 34294726 Free PMC article. Review.
Cited by
-
Pitfalls and promises of bile duct alternatives: A narrative review.World J Gastroenterol. 2022 Oct 21;28(39):5707-5722. doi: 10.3748/wjg.v28.i39.5707. World J Gastroenterol. 2022. PMID: 36338889 Free PMC article. Review.
-
Differential efficacies of marigold leaves and turmeric paste on the healing of the incised wound in sheep.J Adv Vet Anim Res. 2020 Dec 5;7(4):750-757. doi: 10.5455/javar.2020.g477. eCollection 2020 Dec. J Adv Vet Anim Res. 2020. PMID: 33409322 Free PMC article.
-
Pilot Study of the Biological Properties and Vascularization of 3D Printed Bilayer Skin Grafts.Int J Bioprint. 2020 Jan 21;6(1):246. doi: 10.18063/ijb.v6i1.246. eCollection 2020. Int J Bioprint. 2020. PMID: 32596551 Free PMC article.
-
Novel Biotherapeutics Targeting Biomolecular and Cellular Approaches in Diabetic Wound Healing.Biomedicines. 2023 Feb 18;11(2):613. doi: 10.3390/biomedicines11020613. Biomedicines. 2023. PMID: 36831151 Free PMC article. Review.
-
Skin biomechanics: a potential therapeutic intervention target to reduce scarring.Burns Trauma. 2022 Aug 23;10:tkac036. doi: 10.1093/burnst/tkac036. eCollection 2022. Burns Trauma. 2022. PMID: 36017082 Free PMC article. Review.
References
-
- Kiernan JA. Hypotheses concerned with axonal regeneration in the mammalian nervous system. Biol Rev Camb Philos Soc. 1979;54(2):155–97. - PubMed
-
- Vogelaar CF, König B, Krafft S, Estrada V, Brazda N, Ziegler B, et al. Pharmacological Suppression of CNS Scarring by Deferoxamine Reduces Lesion Volume and Increases Regeneration in an In Vitro Model for Astroglial-Fibrotic Scarring and in Rat Spinal Cord Injury In Vivo. PLoS One. 2015;10(7):e0134371. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
