

Placental Stromal Cell Therapy for Experimental Autoimmune Encephalomyelitis: The Role of Route of Cell Delivery
- PMID: 28371563
- PMCID: PMC5442828
- DOI: 10.5966/sctm.2015-0363
Placental Stromal Cell Therapy for Experimental Autoimmune Encephalomyelitis: The Role of Route of Cell Delivery
Abstract
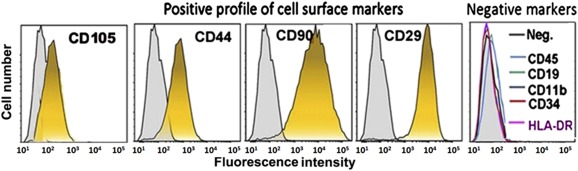
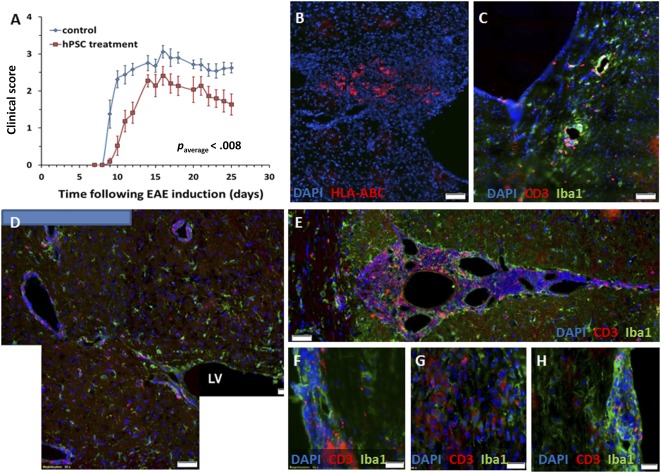
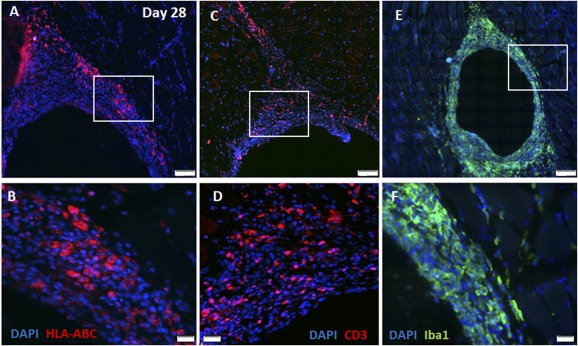
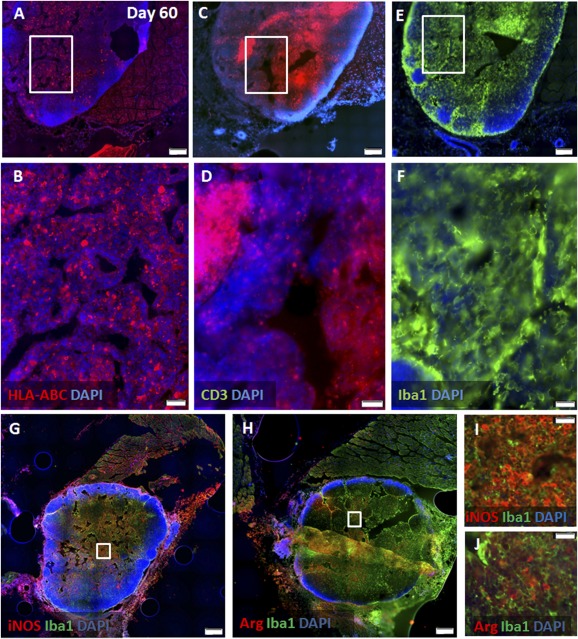
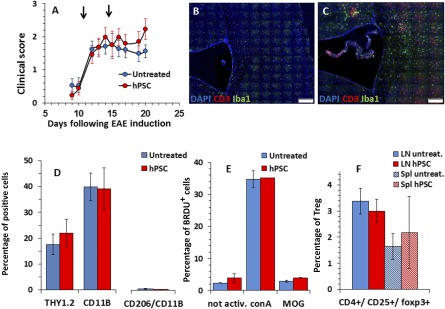
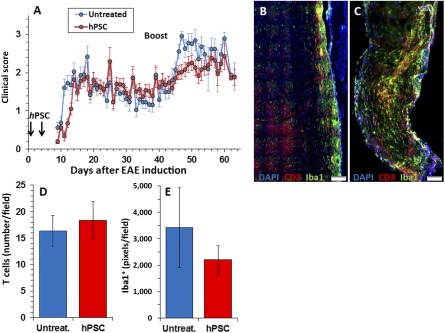
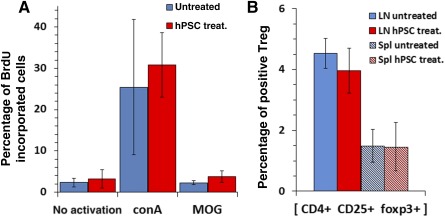
Multiple sclerosis (MS) is an immune-mediated disease of the central nervous system (CNS) with no effective treatment available for the chronic-progressive stage. Cell therapy is a promising therapeutic approach for attenuating the immune-mediated CNS process. Isolated and expanded human placental stromal cells (hPSCs) possess potent immunomodulatory and trophic properties, making them a good candidate for MS therapy. We examined the potential of hPSC therapy in preventing the onset or attenuating the course of established disease in a murine MS model of myelin oligodendrocyte glycoprotein-induced experimental autoimmune encephalomyelitis. We examined the feasibility of hPSC systemic delivery by intramuscular (i.m.) implantation rather than the commonly used intravenous injection, which is dose-limiting and carries the risk of pulmonary obstruction. Our findings showed significant attenuation of the disease only when hPSCs were injected directly to the central nervous system. Intramuscular implanted hPSCs survived at the site of injection for at least 2 months and elicited extensive local immune responses. Intramuscular hPSC implantation before disease onset caused a delay in the appearance of clinical signs and reduced the severity of a relapse induced by repeated challenge with the autoantigen. Intramuscular implantation after disease onset did not affect its course. Thus, pathological analysis of CNS tissue did not show inhibition of neuroinflammation in i.m. hPSC-implanted mice. Moreover, no apparent effect was seen on the proliferative response of peripheral lymph node cells in these animals. We conclude that to maximize their therapeutic potential in MS, hPSCs should be delivered directly to the affected CNS. Stem Cells Translational Medicine 2017;6:1286-1294.
Keywords: Cell therapy; Multiple sclerosis; Placenta; Route of cell delivery.
© 2017 The Authors Stem Cells Translational Medicine published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Figures
References
-
- Einstein O, Fainstein N, Vaknin I et al. Neural precursors attenuate autoimmune encephalomyelitis by peripheral immunosuppression. Ann Neurol 2007;61:209–218. - PubMed
-
- Einstein O, Grigoriadis N, Mizrachi‐Kol R et al. Transplanted neural precursor cells reduce brain inflammation to attenuate chronic experimental autoimmune encephalomyelitis. Exp Neurol 2006;198:275–284. - PubMed
-
- Zappia E, Casazza S, Pedemonte E et al. Mesenchymal stem cells ameliorate experimental autoimmune encephalomyelitis inducing T‐cell anergy. Blood 2005;106:1755–1761. - PubMed
-
- Pluchino S, Martino G. The therapeutic use of stem cells for myelin repair in autoimmune demyelinating disorders. J Neurol Sci 2005;233:117–119. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
