

Mutational burden, immune checkpoint expression, and mismatch repair in glioma: implications for immune checkpoint immunotherapy
- PMID: 28371827
- PMCID: PMC5570198
- DOI: 10.1093/neuonc/nox026
Mutational burden, immune checkpoint expression, and mismatch repair in glioma: implications for immune checkpoint immunotherapy
Abstract
Background: Despite a multiplicity of clinical trials testing immune checkpoint inhibitors, the frequency of expression of potential predictive biomarkers is unknown in glioma.
Methods: In this study, we profiled the frequency of shared biomarker phenotypes. To clarify the relationships among tumor mutational load (TML), mismatch repair (MMR), and immune checkpoint expression, we profiled patients with glioma (n = 327), including glioblastoma (GBM) (n = 198), whose samples had been submitted for analysis from 2009 to 2016. The calculation algorithm for TML included nonsynonymous mutation counts per tumor, with germline mutations filtered out. Immunohistochemical analysis and next-generation sequencing were used to determine tumor-infiltrating lymphocyte expression positive for programmed cell death protein 1 (PD-1), PD ligand 1 (PD-L1) expression on tumor cells, MMR (MLH1, MSH2, MSH6, and PMS2) protein expression and mutations, and DNA polymerase epsilon (POLE) mutations.
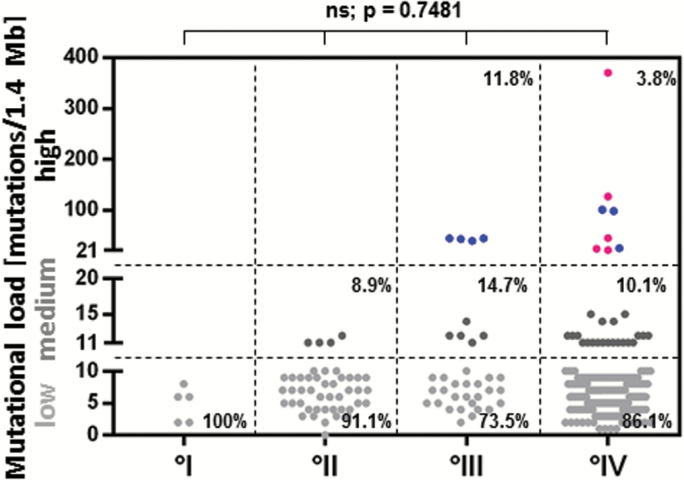
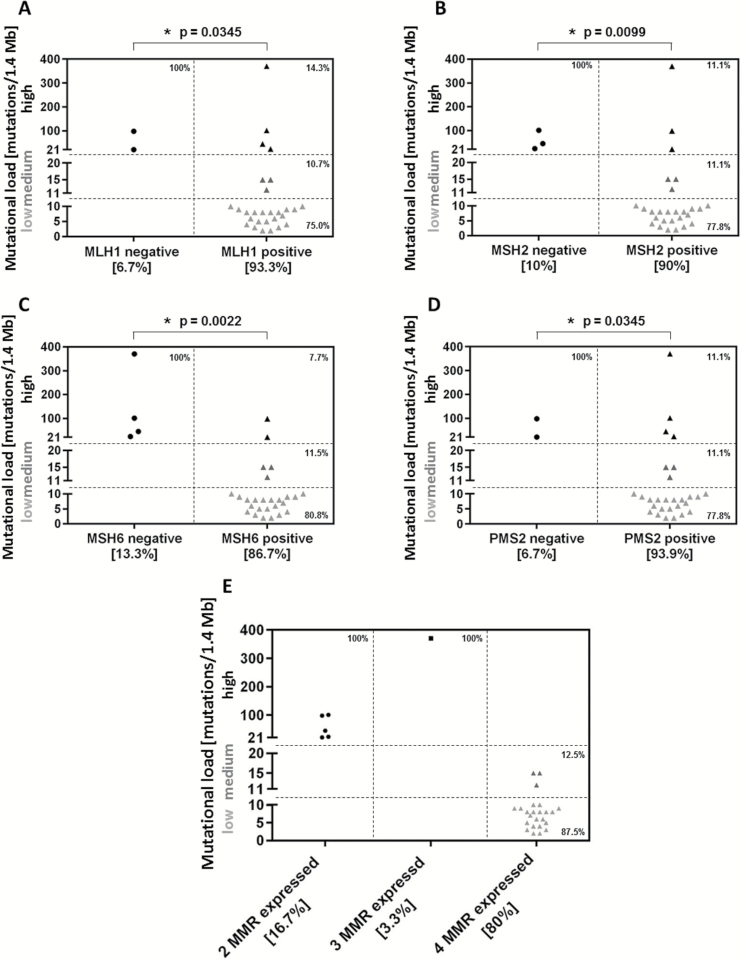
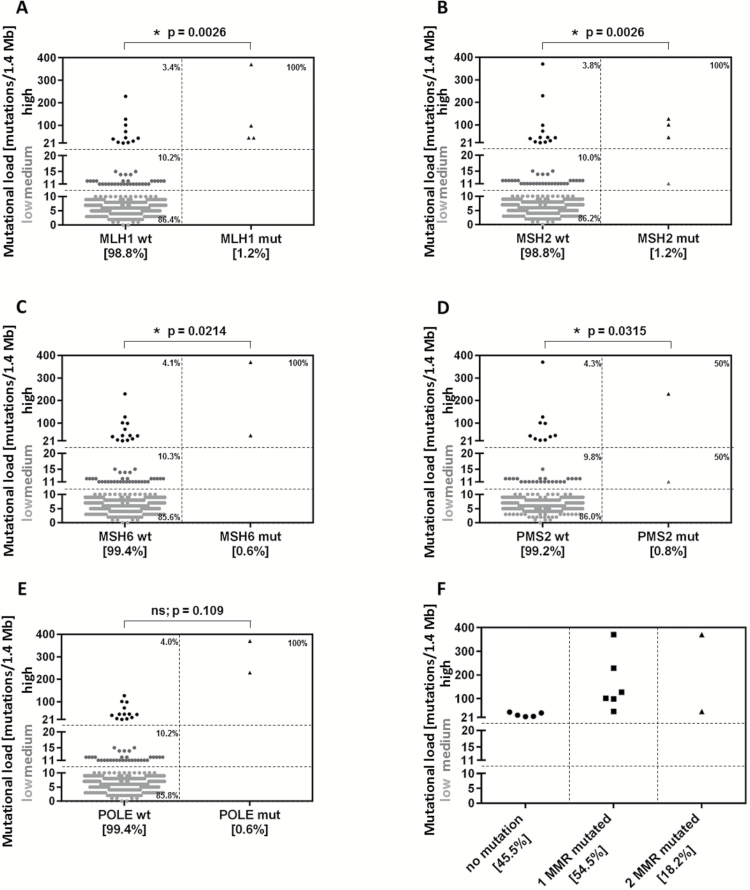
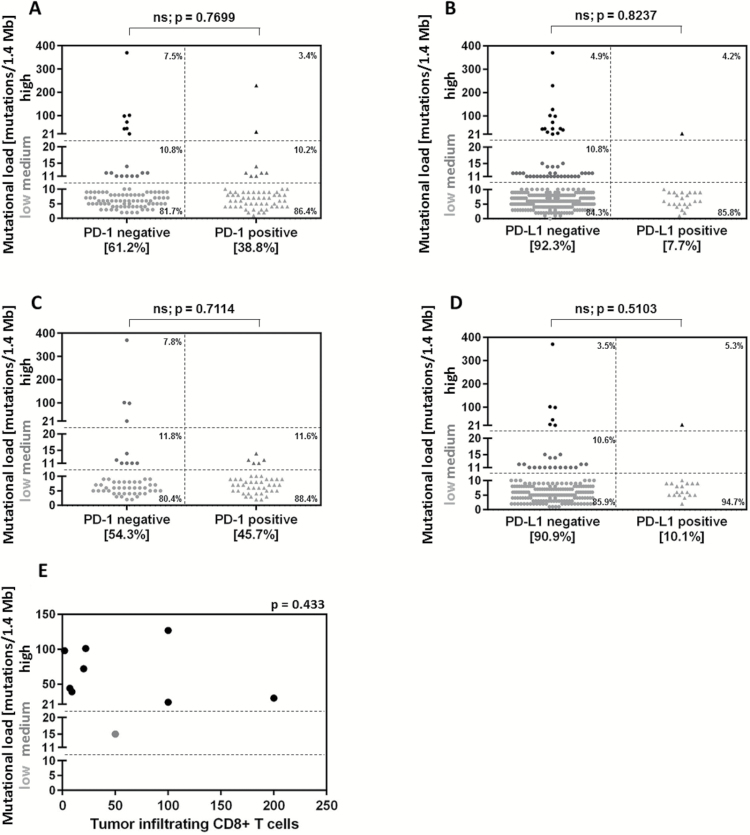
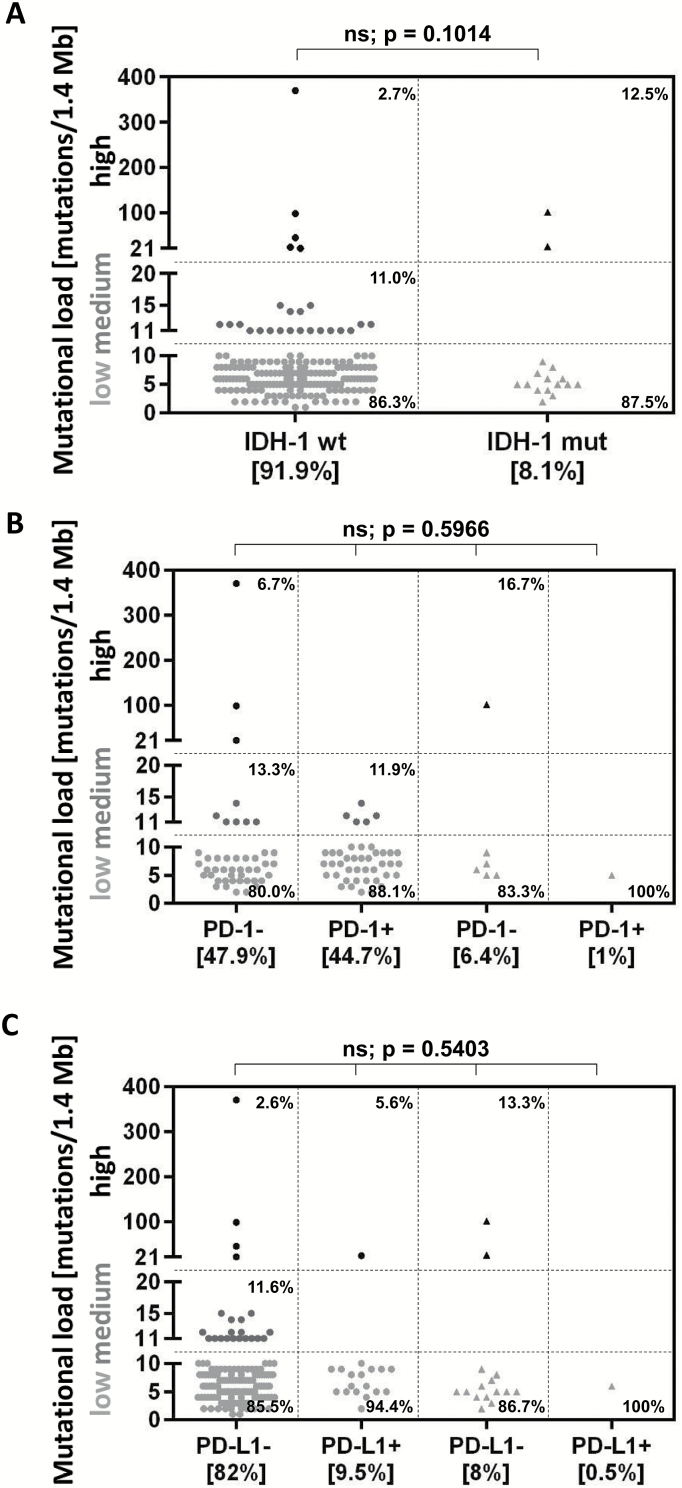
Results: High TML was only found in 3.5% of GBM patients (7 of 198) and was associated with the absence of protein expression of mutL homolog 1 (MLH1) (P = .0345), mutS homolog 2 (MSH2) (P = .0099), MSH6 (P = .0022), and postmeiotic segregation increased 2 (PMS2) (P = .0345) and the presence of DNA MMR mutations. High and moderate TML GBMs did not have an enriched influx of CD8+ T cells, PD-1+ T cells, or tumor-expressed PD-L1. IDH1 mutant gliomas were not enriched for high TML, PD-1+ T cells, or PD-L1 expression.
Conclusions: To clarify the relationships among TML, MMR, and immune checkpoint expression, we profiled the frequency of shared biomarker phenotypes. On the basis of a variety of potential biomarkers of response to immune checkpoints, only small subsets of glioma patients are likely to benefit from monotherapy immune checkpoint inhibition.
Keywords: glioblastoma; glioma; immune checkpoint; mismatch repair; mutational load.
© The Author(s) 2017. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
Figures
References
-
- Weber JS, D’Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16(4):375–384. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
