

Management of Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State
- PMID: 28372715
- PMCID: PMC6535398
- DOI: 10.1016/j.mcna.2016.12.011
Management of Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State
Abstract
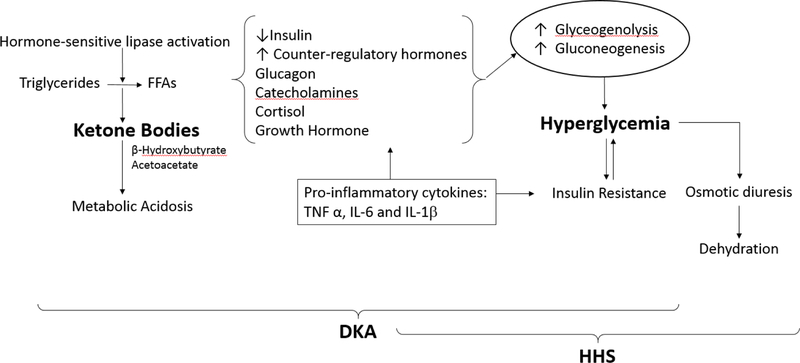
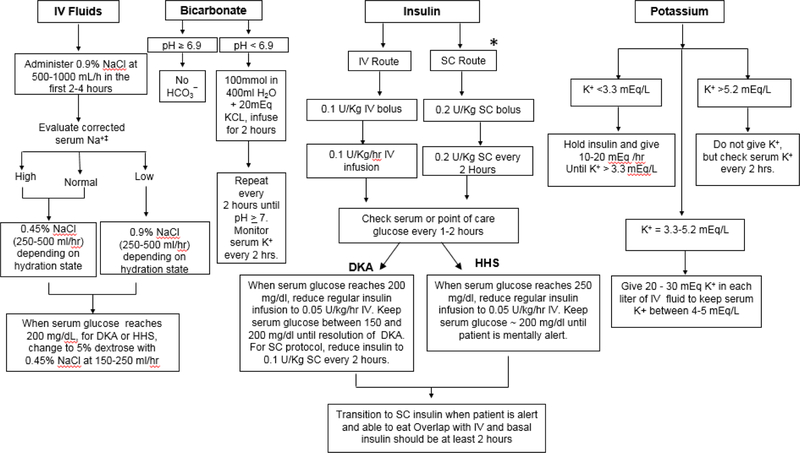
Diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS) are the most serious and life-threatening hyperglycemic emergencies in diabetes. DKA is more common in young people with type 1 diabetes and HHS in adult and elderly patients with type 2 diabetes. Features of the 2 disorders with ketoacidosis and hyperosmolality may coexist. Both are characterized by insulinopenia and severe hyperglycemia. Early diagnosis and management are paramount. Treatment is aggressive rehydration, insulin therapy, electrolyte replacement, and treatment of underlying precipitating events. This article reviews the epidemiology, pathogenesis, diagnosis, and management of hyperglycemic emergencies.
Keywords: Diabetes; Diabetic ketoacidosis; Hyperglycemic emergencies; Hyperglycemic hyperosmolar state; Management of hyperglycemic emergencies.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Centers for Disease Control and Prevention. Mortality due to Hyperglycemic crises http://www.cdc.gov/diabetes/statistics/complications_national.htm. 11/19/2013. Accessed on 9/2/2016.
-
- Ennis ED, Stahl EJVB, Kreisberg RA. The hyperosmolar hyperglycemic syndrome. Diabetes Rev 1994;2:115–126.
-
- Umpierrez GE, Kelly JP, Navarrete JE, Casals MM, Kitabchi AE. Hyperglycemic crises in urban blacks. Arch Intern Med 1997;157(6):669–675. - PubMed
-
- von Stosch A Versuch einer Pathologie und Therapie des Diabetes Mellitus. Berlin, Duncker und Humblot, 1828. [in German].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
