

Myocardial Damage Detected by Late Gadolinium Enhancement Cardiac Magnetic Resonance Is Uncommon in Peripartum Cardiomyopathy
- PMID: 28373243
- PMCID: PMC5533034
- DOI: 10.1161/JAHA.117.005472
Myocardial Damage Detected by Late Gadolinium Enhancement Cardiac Magnetic Resonance Is Uncommon in Peripartum Cardiomyopathy
Abstract
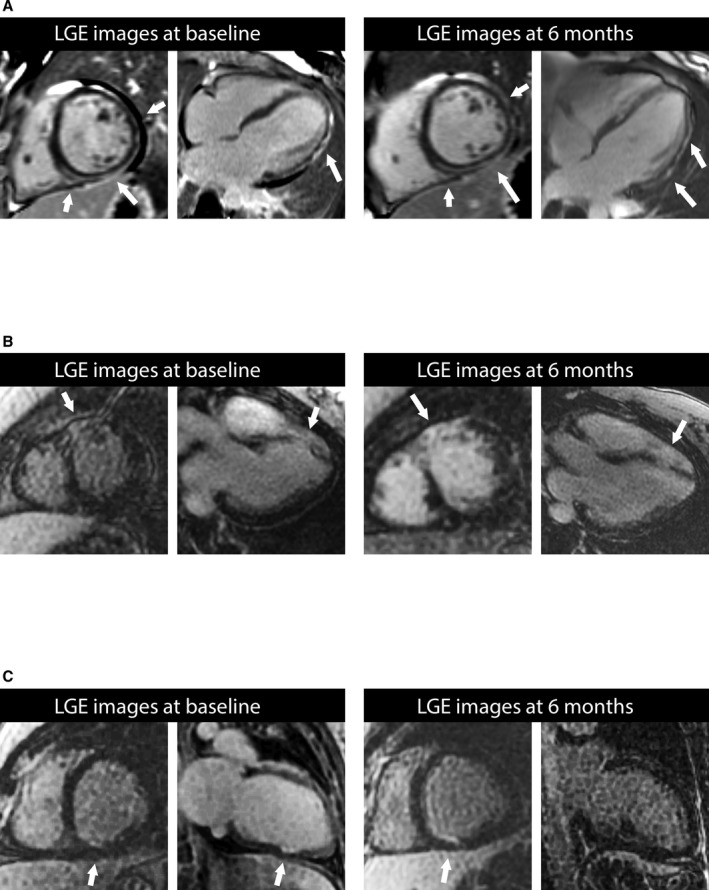
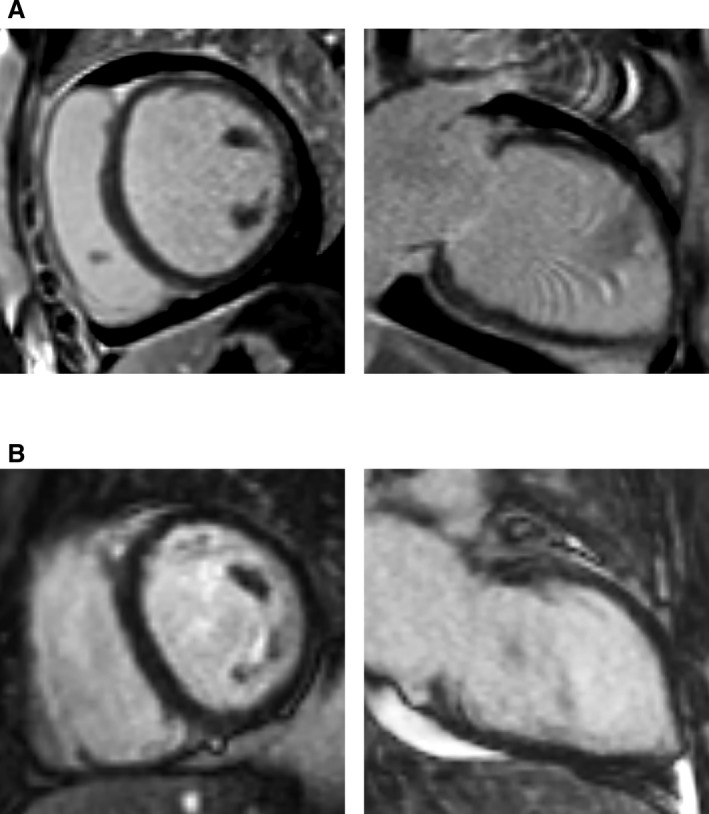
Background: In peripartum cardiomyopathy, the prevalence of focal myocardial damage detected by late gadolinium enhancement (LGE) cardiovascular magnetic resonance is important to elucidate mechanisms of myocardial injury and cardiac dysfunction. LGE equates irreversible myocardial injury, but LGE prevalence in peripartum cardiomyopathy is uncertain.
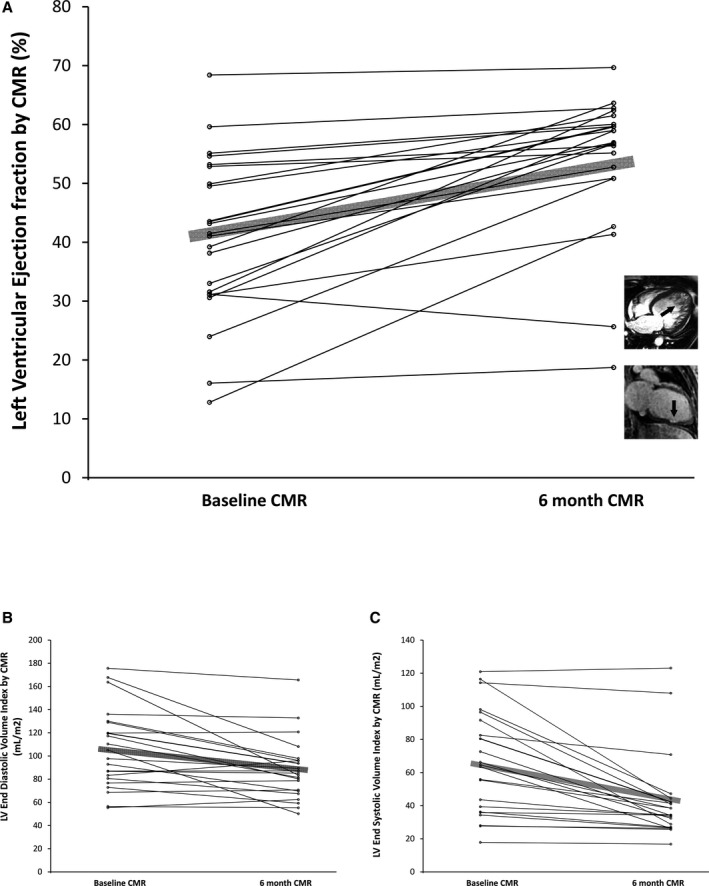
Methods and results: Among 100 women enrolled within the Investigations of Pregnancy Associated Cardiomyopathy cohort, we recruited 40 women at 13 centers to undergo LGE cardiovascular magnetic resonance, enrolled within the first 13 weeks postpartum. Follow-up scans occurred at 6 months postpartum, and death/transplant rates at 12 months. Baseline characteristics did not differ significantly in the parent cohort according to cardiovascular magnetic resonance enrollment except for mechanical circulatory support. LGE was noted only in 2 women (5%) at baseline. While left ventricular dysfunction with enlargement was prevalent at baseline cardiovascular magnetic resonance scans (eg, ejection fraction 38% [Q1-Q3 31-50%], end diastolic volume index=108 mL/m2 [Q1-Q3 83-134 mL/m2]), most women demonstrated significant improvements at 6 months, consistent with a low prevalence of LGE. LGE was not related to baseline clinical variables, ejection fraction, New York Heart Association heart failure class, or mortality. Neither of the 2 women who died exhibited LGE. LGE was inversely associated with persistent left ventricular ejection fraction at 6 months (P=0.006).
Conclusions: Factors other than focal myocardial damage detectable by LGE explain the initial transient depressions in baseline left ventricular ejection fraction, yet focal myocardial damage may contribute to persistent myocardial dysfunction and hinder recovery in a small minority. Most women exhibit favorable changes in ventricular function over 6 months.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01085955.
Keywords: cardiovascular magnetic resonance; heart failure; myocardial fibrosis; peripartum cardiomyopathy; pregnancy and postpartum.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- McNamara DM, Elkayam U, Alharethi R, Damp J, Hsich E, Ewald G, Modi K, Alexis JD, Ramani GV, Semigran MJ, Haythe J, Markham DW, Marek J, Gorcsan J III, Wu WC, Lin Y, Halder I, Pisarcik J, Cooper LT, Fett JD. Clinical outcomes for peripartum cardiomyopathy in North America: results of the IPAC Study (Investigations of Pregnancy‐Associated Cardiomyopathy). J Am Coll Cardiol. 2015;66:905–914. - PMC - PubMed
-
- Elkayam U. Clinical characteristics of peripartum cardiomyopathy in the United States: diagnosis, prognosis, and management. J Am Coll Cardiol. 2011;58:659–670. - PubMed
-
- Haghikia A, Rontgen P, Vogel‐Claussen J, Schwab J, Westenfeld R, Ehlermann P, Berliner D, Podewski E, Hilfiker‐Kleiner D, Bauersachs J. Prognostic implication of right ventricular involvement in peripartum cardiomyopathy: a cardiovascular magnetic resonance study. ESC Heart Fail. 2015;2:139–149. - PMC - PubMed
-
- Gulati A, Jabbour A, Ismail TF, Guha K, Khwaja J, Raza S, Morarji K, Brown TD, Ismail NA, Dweck MR, Di Pietro E, Roughton M, Wage R, Daryani Y, O'Hanlon R, Sheppard MN, Alpendurada F, Lyon AR, Cook SA, Cowie MR, Assomull RG, Pennell DJ, Prasad SK. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA. 2013;309:896–908. - PubMed
-
- Mouquet F, Lions C, de Groote P, Bouabdallaoui N, Willoteaux S, Dagorn J, Deruelle P, Lamblin N, Bauters C, Beregi JP. Characterisation of peripartum cardiomyopathy by cardiac magnetic resonance imaging. Eur Radiol. 2008;18:2765–2769. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
