

Performance and economic evaluation of the molecular detection of pathogens for patients with severe infections: the EVAMICA open-label, cluster-randomised, interventional crossover trial
- PMID: 28374097
- PMCID: PMC5633620
- DOI: 10.1007/s00134-017-4766-4
Performance and economic evaluation of the molecular detection of pathogens for patients with severe infections: the EVAMICA open-label, cluster-randomised, interventional crossover trial
Abstract
Purpose: Microbiological diagnosis (MD) of infections remains insufficient. The resulting empirical antimicrobial therapy leads to multidrug resistance and inappropriate treatments. We therefore evaluated the cost-effectiveness of direct molecular detection of pathogens in blood for patients with severe sepsis (SES), febrile neutropenia (FN) and suspected infective endocarditis (SIE).
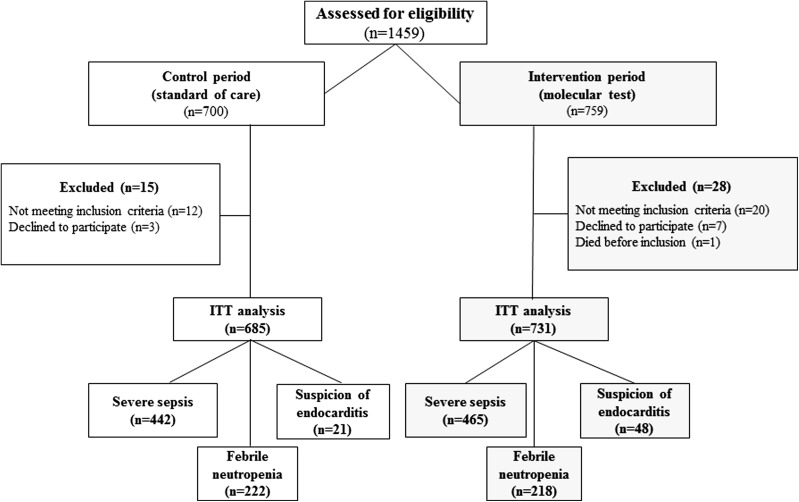
Methods: Patients were enrolled in a multicentre, open-label, cluster-randomised crossover trial conducted during two consecutive periods, randomly assigned as control period (CP; standard diagnostic workup) or intervention period (IP; additional testing with LightCycler®SeptiFast). Multilevel models used to account for clustering were stratified by clinical setting (SES, FN, SIE).
Results: A total of 1416 patients (907 SES, 440 FN, 69 SIE) were evaluated for the primary endpoint (rate of blood MD). For SES patients, the MD rate was higher during IP than during CP [42.6% (198/465) vs. 28.1% (125/442), odds ratio (OR) 1.89, 95% confidence interval (CI) 1.43-2.50; P < 0.001], with an absolute increase of 14.5% (95% CI 8.4-20.7). A trend towards an association was observed for SIE [35.4% (17/48) vs. 9.5% (2/21); OR 6.22 (0.98-39.6)], but not for FN [32.1% (70/218) vs. 30.2% (67/222), P = 0.66]. Overall, turn-around time was shorter during IP than during CP (22.9 vs. 49.5 h, P < 0.001) and hospital costs were similar (median, mean ± SD: IP €14,826, €18,118 ± 17,775; CP €17,828, €18,653 ± 15,966). Bootstrap analysis of the incremental cost-effectiveness ratio showed weak dominance of intervention in SES patients.
Conclusion: Addition of molecular detection to standard care improves MD and thus efficiency of healthcare resource usage in patients with SES. ClinicalTrials.gov registration number: NCT00709358.
Keywords: Aetiological source; Bacteremia; PCR; Sepsis.
Conflict of interest statement
Conflicts of interest
The authors have no conflict of interest within the scope of this study.
Funding
The study was fund by the French Ministry of Health (Grant n°STIC IC0703; P070308 and IDRCB 2007-A01443-50). Clinical research was monitored by the Assistance Publique-Hôpitaux de Paris (AP-HP) institution and particularly the Unité de Recherche Clinique (URC) Mondor. Data basis was collected and stored at URC Mondor. The trial protocol was approved by the institutional ethics committee of Ile-de-France (CPP Ile de France 1 no. 0811715). Written informed consents were obtained for all patients and good practices in clinical research were monitored by the Assistance Publique-Hôpitaux de Paris (AP-HP) institution.
Figures
Comment in
-
Real -time PCR for early microbiological diagnosis: is it time?Intensive Care Med. 2017 Nov;43(11):1714-1716. doi: 10.1007/s00134-017-4793-1. Epub 2017 May 23. Intensive Care Med. 2017. PMID: 28536877 Free PMC article. No abstract available.
References
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent JL, Moreno R. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39:165–228. doi: 10.1007/s00134-012-2769-8. - DOI - PMC - PubMed
-
- Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad, II, Rolston KV, Young JA, Wingard JR, Infectious Diseases Society of A Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52:e56–e93. doi: 10.1093/cid/cir073. - DOI - PubMed
-
- Duval X, Delahaye F, Alla F, Tattevin P, Obadia JF, Le Moing V, Doco-Lecompte T, Celard M, Poyart C, Strady C, Chirouze C, Bes M, Cambau E, Iung B, Selton-Suty C, Hoen B. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: three successive population-based surveys. J Am Coll Cardiol. 2012;59:1968–1976. doi: 10.1016/j.jacc.2012.02.029. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
